Primary hyperaldosteronism, also known as Conn’s syndrome, is a condition where the adrenal glands release too much aldosterone.
What is primary hyperaldosteronism?
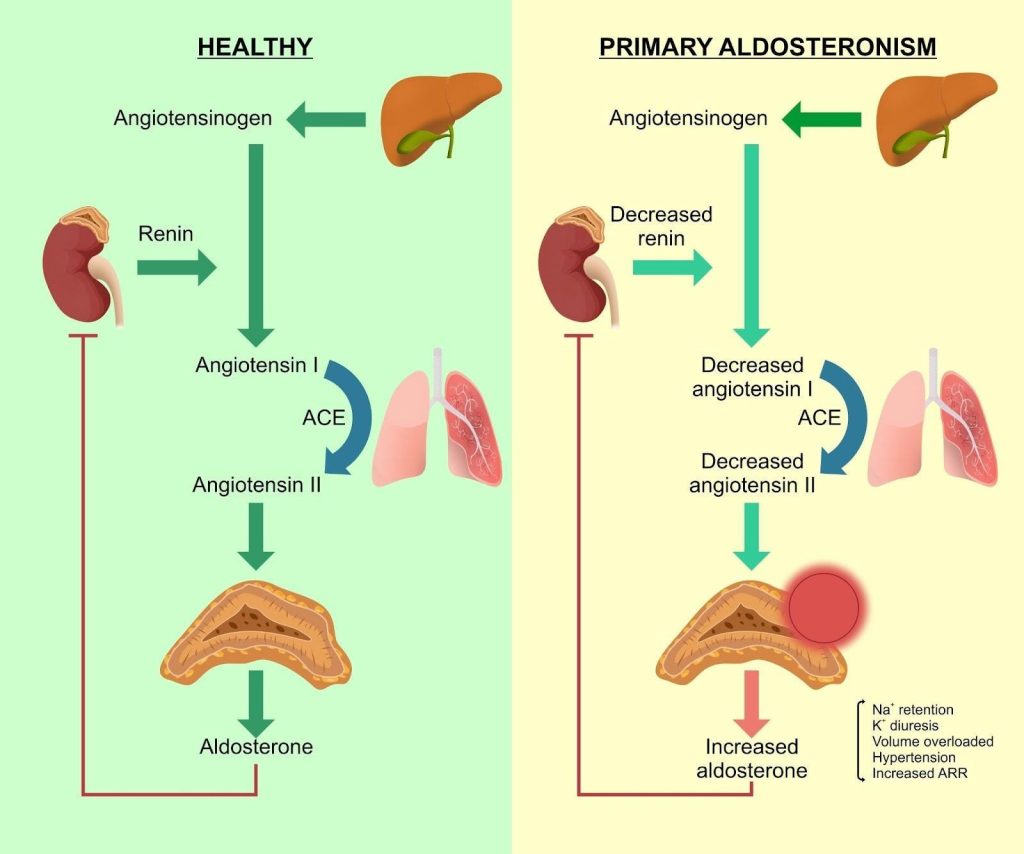
Primary hyperaldosteronism, also known as Conn’s syndrome, is a condition where the adrenal glands release too much aldosterone. Aldosterone is a hormone that helps the body balance salt and water by controlling how much sodium is retained and how much potassium is removed by the kidneys. In primary hyperaldosteronism, this hormone is produced in excess without regulation.
The result is that the kidneys hold on to more sodium and water than the body needs, increasing blood volume and raising blood pressure. At the same time, too much potassium is lost in the urine, which can lead to low potassium levels in the blood (hypokalaemia). While it can occur at any age, primary hyperaldosteronism is an important cause of high blood pressure in younger adults and is a recognised contributor to resistant hypertension, where blood pressure remains high despite the use of standard medications. It has been shown to be the cause of 5 percent of hypertension and is reversible.
Primary hyperaldosteronism is a condition where the adrenal glands produce excess aldosterone independently of the renin–angiotensin system, causing sodium retention, potassium loss, and high blood pressure.
What causes primary hyperaldosteronism?
Primary hyperaldosteronism develops when one or both adrenal glands produce aldosterone in an uncontrolled way. The most common causes are:
Less common causes include a single enlarged adrenal gland without a visible tumour, cancer of the adrenal gland, or inherited forms where genetic changes cause the adrenal tissue to overproduce aldosterone.
Regardless of the cause, the overproduction is “primary” because it originates in the adrenal glands themselves, rather than being driven by another condition elsewhere in the body. Identifying the underlying cause is important, as treatment may differ depending on whether one or both glands are involved.
What are the signs and symptoms of primary hyperaldosteronism?
Primary hyperaldosteronism does not always cause obvious symptoms, and some people are diagnosed only after routine blood pressure checks or blood tests. The condition’s effects come mainly from two factors: raised blood pressure and low potassium levels.
Common signs and symptoms include:
High blood pressure — often moderate to severe and sometimes resistant to standard medication. In younger adults, it may appear earlier than expected for essential hypertension.
Low blood potassium (hypokalaemia) — not always present, but when it occurs it can cause:
Muscle weakness or cramps
Fatigue or low energy
Tingling sensations or numbness
Palpitations or irregular heartbeat
Frequent urination and excessive thirst — caused by the body’s altered salt and water balance.
Headaches or blurred vision — sometimes linked to persistently high blood pressure.
In many cases, people feel well and have no symptoms apart from raised blood pressure, which is why screening for primary hyperaldosteronism is important in certain groups, particularly younger patients with unexplained or resistant hypertension.
Who is at risk of primary hyperaldosteronism in Singapore?
Primary hyperaldosteronism can occur in many different patient groups, but some are at a higher likelihood of having the condition. In Singapore, these risk factors are consistent with international guidelines, and recognising them is important for early detection and treatment.
Sustained high blood pressure — people with consistently elevated blood pressure, particularly readings above 140/90 mmHg on several occasions, are more likely to have underlying primary hyperaldosteronism compared to those with mild hypertension.
Resistant hypertension — this refers to blood pressure that remains above target despite taking three antihypertensive medicines, or blood pressure that can only be controlled with four or more medications. This group has a notably higher prevalence of primary hyperaldosteronism.
Low potassium levels (hypokalaemia) — whether caused by the condition itself or triggered by diuretic use, low potassium alongside hypertension is a classic feature that should prompt testing.
Adrenal incidentaloma — an adrenal mass found on scans done for unrelated reasons can sometimes be the source of excess aldosterone production, even in patients without obvious symptoms.
What complications can arise if primary hyperaldosteronism is left untreated?
Without proper treatment, primary hyperaldosteronism can lead to serious long-term health problems. Persistent excess aldosterone not only keeps blood pressure high but also directly damages the heart, blood vessels, and kidneys.
Cardiovascular disease — long-standing high blood pressure and aldosterone excess increase the risk of heart attack, heart failure, atrial fibrillation, and stroke. These risks are higher than in people with essential hypertension of the same severity.
Electrolyte imbalance — untreated hypokalaemia can result in muscle weakness, cramps, fatigue, and dangerous heart rhythm disturbances.
Increased mortality — studies have shown that people with untreated primary hyperaldosteronism have higher rates of cardiovascular and kidney-related deaths compared to those with high blood pressure from other causes. Dr. Dinesh says Primary hyperaldosteronism confers a higher risk than usual and that makes the case for its detection and potential cure.
Reduced quality of life — persistent symptoms such as headaches, palpitations, and muscle weakness can affect daily activities, work performance, and overall well-being.
How is primary hyperaldosteronism diagnosed?
Diagnosing primary hyperaldosteronism involves confirming that the adrenal glands are producing excess aldosterone and determining the underlying cause. This process usually takes place in stages, beginning with screening tests and followed by confirmatory assessments.
Screening with aldosterone-to-renin ratio — a blood test measures the level of aldosterone and renin, then calculates the ratio between them. A high ratio, particularly when renin is suppressed, suggests autonomous aldosterone production and warrants further evaluation.
Confirmatory testing — if the screening test is positive, additional tests are performed to confirm the diagnosis. These usually involve saline infusion. Each assesses whether aldosterone levels remain high when they should normally be suppressed.
Identifying the source — once the diagnosis is confirmed, imaging such as a CT scan of the adrenal glands is used to check for adenomas or enlargement. However, imaging alone cannot always distinguish between unilateral and bilateral disease.
Adrenal vein sampling — in many cases, blood samples are taken directly from each adrenal vein to compare aldosterone production between the two glands. This is commonly used for deciding whether surgery or medical therapy is more appropriate.
Additional tests — blood tests to assess potassium levels and kidney function, as well as other hormonal measurements, may be done to guide treatment planning and monitor overall health.
What are the long-term effects of primary hyperaldosteronism?
If primary hyperaldosteronism is not diagnosed and treated early, the continued excess of aldosterone can have lasting effects on multiple organ systems. These effects result from both sustained high blood pressure and the direct harmful actions of aldosterone on the heart, blood vessels, and kidneys.
Heart and blood vessels — chronic exposure to high aldosterone levels can cause thickening of the heart muscle (left ventricular hypertrophy), stiffening of blood vessels, and increased risk of heart rhythm problems such as atrial fibrillation. Over time, this significantly raises the chance of heart attack, stroke, and heart failure.
Kidneys — excess aldosterone promotes scarring and loss of kidney tissue, leading to a gradual decline in kidney function. This may progress to chronic kidney disease, even in people whose blood pressure is well controlled later on.
Metabolic changes — aldosterone excess may contribute to insulin resistance and impaired glucose metabolism, which could increase the risk of developing type 2 diabetes.
Electrolyte-related problems — persistent low potassium can cause long-standing muscle weakness, fatigue, and in severe cases, irreversible heart rhythm disturbances.
Overall life expectancy — people with untreated primary hyperaldosteronism have a higher risk of premature death from cardiovascular and kidney causes compared to those with other types of high blood pressure, making timely diagnosis and treatment essential.
What are the treatment options for primary hyperaldosteronism in Singapore?
Treatment for primary hyperaldosteronism aims to correct the excess aldosterone production, normalise blood pressure, restore potassium balance, and reduce long-term cardiovascular and kidney risks. The approach depends on whether one or both adrenal glands are affected.
Surgical removal (adrenalectomy) — if the excess aldosterone comes from a single adrenal gland, such as with an aldosterone-producing adenoma, surgery to remove the affected gland is often recommended. This can potentially cure the condition or significantly improve blood pressure control.
Medication therapy — when both adrenal glands are overactive, or if surgery is not suitable, treatment involves medicines called mineralocorticoid receptor antagonists, such as spironolactone or eplerenone. These block the effects of aldosterone, helping lower blood pressure and maintain normal potassium levels.
Lifestyle measures — reducing dietary sodium, maintaining a healthy weight, staying physically active, and following other heart-healthy habits can support medical or surgical treatment in controlling blood pressure.
Monitoring and follow-up — regular check-ups, blood pressure monitoring, and periodic blood tests for potassium and kidney function are important to ensure the treatment remains effective and well-tolerated.
Summary
Primary hyperaldosteronism is a hormonal condition where the adrenal glands produce excess aldosterone, leading to high blood pressure and sometimes low potassium levels. It can be caused by an adrenal growth, enlargement of one or both glands, or inherited factors, and is a significant cause of hypertension in younger adults.
If you are experiencing persistent high blood pressure, especially at a young age, or have been told you have low potassium, schedule a consultation with us for a thorough assessment and tailored treatment plan.
Yes. Hormonal changes from primary hyperaldosteronism can affect the nervous system, sometimes leading to irritability, anxiety, or mood swings, particularly when potassium levels drop.
In many cases, yes. If it’s caused by a single overactive adrenal gland, surgery can cure primary hyperaldosteronism. For bilateral disease, medication can control symptoms and prevent long-term damage.
No. While low potassium is a classic sign, many people with primary hyperaldosteronism have normal potassium levels, which means the condition can go undiagnosed without proper screening.
Yes. Primary hyperaldosteronism during pregnancy can make blood pressure harder to control and may increase risks for both mother and baby, so close monitoring by a specialist is important.
Some rare types of primary hyperaldosteronism are inherited due to genetic changes. If a close family member has the condition, screening may be recommended even without symptoms.
A low-salt diet supports treatment for primary hyperaldosteronism by helping control blood pressure and reducing fluid retention, though it cannot replace medical or surgical therapy.
Blood pressure may improve within weeks after surgery or starting medication for primary hyperaldosteronism, but full stabilisation can take several months.
Recurrence is rare after successful surgery for primary hyperaldosteronism, but ongoing follow-up is important to monitor blood pressure and hormone levels, especially in bilateral disease.
Yes. Even with similar blood pressure readings, people with untreated primary hyperaldosteronism have a higher risk of stroke compared to those with essential hypertension, due to the direct harmful effects of aldosterone.
chat with us
Welcome to The Metabolic Clinic
Holistic Care for Hormones, Bones, and Metabolic Health
Dr Dinesh graduated with honours from Monash University, Melbourne in 2009, receiving the Prince Henry's Prize in Surgery. During his endocrinology training in Melbourne, he won the top registrar award at the Endocrine Society of Australia Clinical Weekend in 2016, followed by securing Australia's only Andrology fellowship in 2017. Upon returning to Singapore, he was the sub-speciality lead for adrenal, pituitary, and bone services at Khoo Teck Puat Hospital and established The Metabolic Bone Clinic.
A passionate educator, he served as Associate Programme Director for Endocrinology at NHG, training the next generation of endocrinologists, and received the NHG Teaching Award for Senior Doctors in 2023. An expert endocrinologist with proficiency in both general and sub-speciality endocrinology, he has an interest in longevity through improving cardiovascular risk, metabolism, bone health, and muscle loss prevention, with the ultimate aim of improving the number of healthy years in one's life.
10+ Years of Experience in Hormone & Metabolic Health
Founder of The Metabolic Bone Clinic in Khoo Teck Puat Hospital
Sub-specialist training with international experts in Melbourne, Australia
Clinical Interest in Longevity & Metabolic Health
START YOUR PERSONALISED HEALTH JOURNEY
If you’re not achieving your treatment targets, struggling with weight changes, fatigue, or unexplained symptoms—it’s time to take a deeper look.
Get clarity with a tailored plan built around you and improving your metabolic health.