Adrenal insufficiency, commonly referred to as Addison’s disease when it is in origin, is a rare but serious condition in which the adrenal glands fail to produce adequate levels of essential hormones.
Adrenal insufficiency, commonly referred to as Addison’s disease when it is in origin, is a rare but serious condition in which the adrenal glands fail to produce adequate levels of essential hormones, most notably cortisol and, in many cases, aldosterone. These hormones play a critical role in regulating metabolism, blood pressure, immune response, and the body’s reaction to stress. When hormone levels drop too low, even everyday activities can lead to fatigue, dizziness, low blood pressure, and, in severe cases, life-threatening adrenal crises.
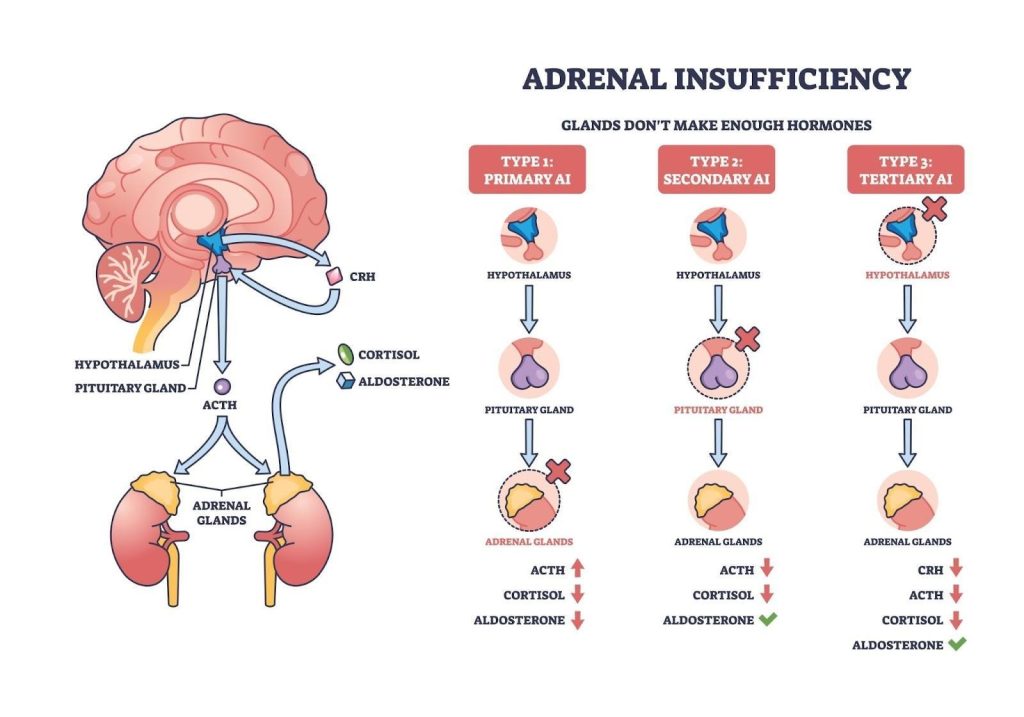
The condition may develop gradually and remain unnoticed for months until symptoms become severe. It can affect individuals of any age or gender, though it is most commonly diagnosed in adults between the ages of 30 and 50. Adrenal insufficiency is broadly categorised into three types:
Tertiary adrenal insufficiency — resulting from suppression of the hypothalamus, often due to long-term use of corticosteroids.
Understanding the type and cause of adrenal insufficiency is essential for appropriate treatment, which usually involves lifelong hormone replacement therapy. With proper medical care and regular monitoring, most individuals can lead healthy and active lives.
Adrenal insufficiency is a condition where the adrenal glands do not produce enough cortisol, and sometimes aldosterone, due to problems in the adrenal glands, pituitary gland, or hypothalamus.
What causes Addison’s disease?
Addison’s disease, or primary adrenal insufficiency, occurs when the adrenal glands are damaged and can no longer produce enough of the essential hormones cortisol and aldosterone. This usually happens gradually and may go unnoticed until symptoms become more pronounced. Several conditions can lead to this adrenal gland dysfunction.
Autoimmune destruction — in most cases, Addison’s disease is caused by autoimmune adrenalitis. Here, the body’s immune system mistakenly attacks the adrenal cortex, progressively destroying the tissue responsible for hormone production. It is often linked to other autoimmune conditions like type 1 diabetes, autoimmune thyroid disease, and vitiligo, and may form part of a broader autoimmune polyglandular syndrome.
Infections — infectious diseases, particularly tuberculosis (TB), remain a major cause of Addison’s disease in developing regions. TB bacteria can invade the adrenal glands, causing them to deteriorate over time. Other infections such as HIV, CMV, and certain fungal infections can also damage adrenal tissue and lead to hormone deficiency.
Adrenal bleeding or infarction — adrenal glands can be damaged rapidly due to haemorrhage (bleeding) or infarction (loss of blood supply). This is seen in cases of severe sepsis, clotting disorders, or conditions like Waterhouse-Friderichsen syndrome. Such events can trigger an abrupt adrenal crisis and require emergency care. Dr. Dinesh says being on blood thinners is a major risk factor.
Cancer and infiltrative diseases — in rare instances, cancers such as lung or breast cancer may spread to the adrenal glands. Other infiltrative diseases like amyloidosis or sarcoidosis can also impair adrenal function by replacing normal gland tissue with abnormal deposits.
What are the symptoms of Addison’s disease?
Symptoms of Addison’s disease tend to develop slowly over weeks or months and may initially be vague or mistaken for other conditions. However, as hormone levels continue to decline, the symptoms become more noticeable and disabling. In some cases, symptoms can worsen suddenly, leading to an adrenal crisis, which is a medical emergency.
Chronic fatigue and muscle weakness — individuals with Addison’s disease often feel persistently tired, even after rest. This fatigue is usually accompanied by muscle weakness, especially in the legs and arms, due to the body’s reduced ability to maintain energy balance.
Weight loss and loss of appetite — unintended weight loss is a hallmark symptom, often due to a combination of reduced appetite, nausea, and gastrointestinal discomfort. Many patients report difficulty eating or maintaining their usual food intake.
Low blood pressure — cortisol and aldosterone help regulate blood pressure. Their deficiency can lead to hypotension, especially postural hypotension (a drop in blood pressure when standing), which causes dizziness, lightheadedness, or fainting.
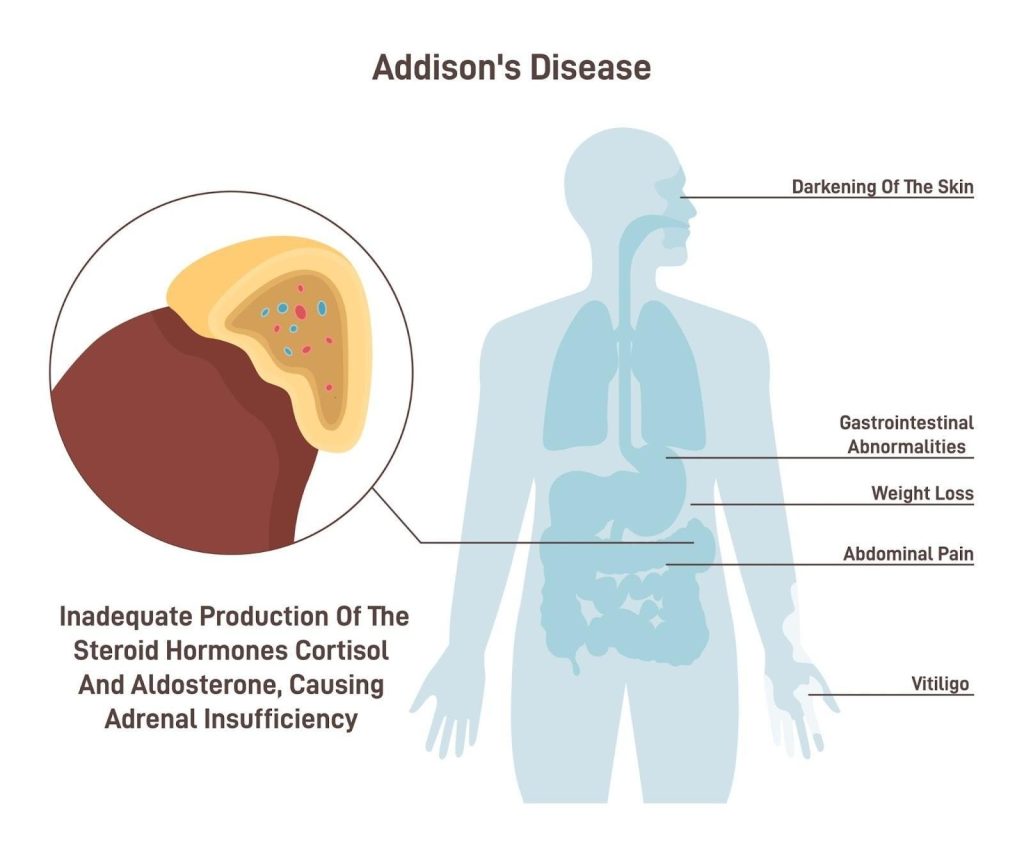
Skin darkening (hyperpigmentation) — in Addison’s disease, high levels of ACTH stimulate melanin production, leading to dark patches on the skin, particularly around scars, skin folds, gums, and pressure points like elbows and knees. This symptom is more specific to primary adrenal insufficiency and may not occur in secondary or tertiary forms.
Salt cravings — people with Addison’s disease often crave salty foods due to the loss of sodium in urine, a result of aldosterone deficiency. This can be accompanied by dehydration and frequent urination.
Nausea, vomiting, and abdominal pain — digestive symptoms such as nausea, vomiting, abdominal cramps, and diarrhoea are common. These may worsen during periods of stress or illness.
Mood changes — low cortisol levels can affect mental health, leading to symptoms like low mood, irritability, and difficulty concentrating. In some cases, people may experience apathy or even cognitive slowing.
Menstrual changes and reduced libido — in women, Addison’s disease can lead to irregular or absent menstrual periods and reduced libido. This is partly due to adrenal involvement in sex hormone production.
Addison’s disease is caused by inadequate production of cortisol and aldosterone, leading to symptoms such as skin darkening, abdominal pain, gastrointestinal disturbances, weight loss, and vitiligo.
Who is at risk of Addison’s disease in Singapore?
Although Addison’s disease is relatively rare, certain individuals are more likely to develop it due to genetic, medical, or environmental factors. Recognising these risk factors can help prompt earlier diagnosis and intervention.
People with autoimmune conditions — individuals who already have an autoimmune disorder, such as type 1 diabetes, autoimmune thyroid disease (Hashimoto’s or Graves’), or vitiligo, are at higher risk of developing Addison’s disease. This is because autoimmune adrenalitis, where the immune system attacks the adrenal glands, is the leading cause of Addison’s in many developed countries.
People with tuberculosis or certain infections — in regions where tuberculosis (TB) is common, individuals with TB infection are at risk, as the bacteria can directly invade and damage the adrenal glands. Other infections like HIV, fungal diseases, and cytomegalovirus (CMV) may also contribute.
Individuals on long-term steroid therapy — those who take corticosteroids (like prednisone) for an extended period may develop secondary adrenal insufficiency, particularly if the medication is stopped abruptly. This happens when the body’s natural cortisol production is suppressed due to external steroid use.
Patients with adrenal surgery or cancer — people who have had adrenal glands surgically removed or affected by cancer (either primary adrenal tumours or metastases) are also at risk. Additionally, those with infiltrative diseases like amyloidosis or sarcoidosis may experience adrenal dysfunction.
Men with adrenoleukodystrophy (ALD) — this X-linked genetic disorder affects the adrenal glands and nervous system, typically in boys and young men. ALD can lead to progressive adrenal insufficiency and neurological decline.
Identifying at-risk individuals helps clinicians monitor for early signs of adrenal insufficiency and initiate timely treatment to avoid complications like adrenal crisis.
How is Addison’s disease diagnosed?
Diagnosing Addison’s disease involves a combination of blood tests, hormone stimulation tests, and imaging studies to confirm adrenal insufficiency and determine its cause. Since early symptoms are often vague and non-specific, a thorough diagnostic approach is essential to avoid delayed or missed diagnosis.
Blood tests — basic blood tests may reveal low levels of cortisol and sodium, high potassium, and elevated ACTH levels. These findings raise suspicion of primary adrenal insufficiency. In secondary adrenal insufficiency, cortisol is low but ACTH is also low or inappropriately normal.
ACTH stimulation test — the short Synacthen (ACTH) stimulation test is the most common test for confirming Addison’s disease. It measures how well the adrenal glands respond to synthetic ACTH. In Addison’s disease, cortisol levels will remain low despite stimulation, which helps confirm the diagnosis.
Renin and aldosterone levels — to evaluate aldosterone production, doctors often check plasma renin activity and aldosterone levels. High renin and low aldosterone suggest mineralocorticoid deficiency, which is typically seen in primary adrenal insufficiency but not in secondary or tertiary forms.
Autoantibody testing — if Addison’s disease is suspected to be autoimmune in origin, specific blood tests can detect adrenal cortex antibodies or 21-hydroxylase antibodies. A positive result supports the diagnosis of autoimmune adrenalitis.
Imaging studies — a CT scan of the adrenal glands may be done to look for enlargement, shrinkage, calcification, or masses. This helps identify causes like tuberculosis, bleeding, or metastatic cancer. In cases of secondary adrenal insufficiency, MRI of the pituitary gland may be recommended.
Accurate diagnosis is vital not only for confirming Addison’s disease but also for determining the underlying cause and guiding appropriate treatment. Early identification reduces the risk of adrenal crisis and improves long-term outcomes.
What are the treatment options for Addison’s disease in Singapore?
The primary goal of treatment for Addison’s disease is to replace the missing hormones — mainly cortisol and, when necessary, aldosterone — to restore balance in the body. With appropriate lifelong hormone replacement and medical supervision, most patients can live normal, active lives.
Glucocorticoid replacement — the primary treatment for Addison’s disease is daily glucocorticoid therapy, most commonly using hydrocortisone. Alternatives like prednisolone or dexamethasone may also be used depending on patient needs. The dosage is typically split into two or three doses per day to mimic the body’s natural cortisol rhythm.
Mineralocorticoid replacement — patients with primary adrenal insufficiency also require fludrocortisone to replace aldosterone, which helps regulate blood pressure and sodium-potassium balance. The dose may be adjusted based on blood pressure, electrolytes, and plasma renin levels.
Salt supplementation — some patients, particularly those with high sodium loss, may be advised to increase their salt intake, especially during periods of heat, heavy sweating, or diarrhoea.
Stress dosing — during periods of physical stress, such as infections, surgery, or trauma, the body normally produces more cortisol. People with Addison’s disease must increase their glucocorticoid dose (“stress dosing”) to prevent adrenal crisis. Patients are often given written instructions and should know how and when to obtain emergency hydrocortisone injections if needed.
Emergency treatment for adrenal crisis — an adrenal crisis is a medical emergency requiring immediate treatment with intravenous hydrocortisone, fluids, and electrolytes. It may present with severe hypotension, vomiting, confusion, or collapse. Rapid recognition and treatment are critical.
Medical alert identification — patients are encouraged to wear a medical alert bracelet or carry a steroid emergency card that informs healthcare professionals of their condition and need for urgent steroid treatment in emergencies.
Regular monitoring — routine follow-up with an endocrinologist helps adjust medication dosages, monitor blood pressure and electrolyte levels, and assess overall health. Hormone needs may change with age, weight fluctuations, or lifestyle changes.
With proper hormone replacement, education, and preparedness for emergencies, most individuals with Addison’s disease can maintain good health and prevent complications.
Summary
Addison’s disease, or primary adrenal insufficiency, is a rare but serious condition in which the adrenal glands fail to produce enough cortisol and aldosterone — hormones essential for regulating stress response, metabolism, blood pressure, and fluid balance. It is most often caused by autoimmune damage, but infections, genetic disorders and other factors can also lead to adrenal failure. Symptoms tend to develop gradually and include fatigue, weight loss, low blood pressure, skin darkening, salt cravings, and mood changes.
Diagnosis involves blood tests, hormone stimulation tests, and imaging to confirm hormone deficiency and identify the underlying cause. Treatment focuses on lifelong hormone replacement and stress management, with proper monitoring to prevent adrenal crisis and support daily well-being.
If you are experiencing unexplained fatigue, low blood pressure, or other symptoms of adrenal insufficiency, schedule a consultation with us for a comprehensive evaluation and personalised treatment plan.
Addison’s disease is a long-term condition of adrenal hormone deficiency. An adrenal crisis is a sudden, life-threatening worsening of the disease that requires emergency treatment.
Addison’s disease is usually confirmed through blood tests, an ACTH stimulation test, and imaging of the adrenal glands to assess their function and structure.
Addison’s disease results from too little cortisol, while Cushing’s syndromeis caused by too much. Their symptoms and hormone levels are opposite in nature.
Dr Dinesh graduated with honours from Monash University, Melbourne in 2009, receiving the Prince Henry's Prize in Surgery. During his endocrinology training in Melbourne, he won the top registrar award at the Endocrine Society of Australia Clinical Weekend in 2016, followed by securing Australia's only Andrology fellowship in 2017. Upon returning to Singapore, he was the sub-speciality lead for adrenal, pituitary, and bone services at Khoo Teck Puat Hospital and established The Metabolic Bone Clinic.
A passionate educator, he served as Associate Programme Director for Endocrinology at NHG, training the next generation of endocrinologists, and received the NHG Teaching Award for Senior Doctors in 2023. An expert endocrinologist with proficiency in both general and sub-speciality endocrinology, he has an interest in longevity through improving cardiovascular risk, metabolism, bone health, and muscle loss prevention, with the ultimate aim of improving the number of healthy years in one's life.
10+ Years of Experience in Hormone & Metabolic Health
Founder of The Metabolic Bone Clinic in Khoo Teck Puat Hospital
Sub-specialist training with international experts in Melbourne, Australia
Clinical Interest in Longevity & Metabolic Health
START YOUR PERSONALISED HEALTH JOURNEY
If you’re not achieving your treatment targets, struggling with weight changes, fatigue, or unexplained symptoms—it’s time to take a deeper look.
Get clarity with a tailored plan built around you and improving your metabolic health.