Aldosterone excess can cause muscle cramps or weakness due to low potassium levels affecting normal muscle function.
Aldosterone suppression refers to the medical management of conditions where the body produces too much aldosterone. Excess aldosterone is a recognised and treatable cause of secondary hypertension and can significantly increase cardiovascular risk if left unaddressed. It is thought to account for 5 to 10 percent of all hypertension and is reversible.
Because its effects are often silent in the early stages, many people are diagnosed only during evaluation for resistant high blood pressure or unexplained low potassium levels. Targeted testing allows clinicians to identify the cause and initiate appropriate treatment to restore hormonal balance.It is important to treat because the hypertension from primary hyperaldosteronism causes more heart attacks and strokes than normal stock-standard ‘essential hypertension’.
What is aldosterone?
Aldosterone is a mineralocorticoid steroid hormone produced by the adrenal glands that plays a central role in regulating blood pressure, sodium balance and potassium levels. It signals the kidneys to retain sodium and water while excreting potassium. This process helps maintain blood volume and stable circulation.
When aldosterone is produced in excess, the body retains too much sodium and loses too much potassium. This can result in persistent or difficult-to-control high blood pressure, low potassium levels and long-term cardiovascular strain. Identifying and treating aldosterone excess early is important to reduce complications and protect heart and kidney health.
What is aldosterone excess?
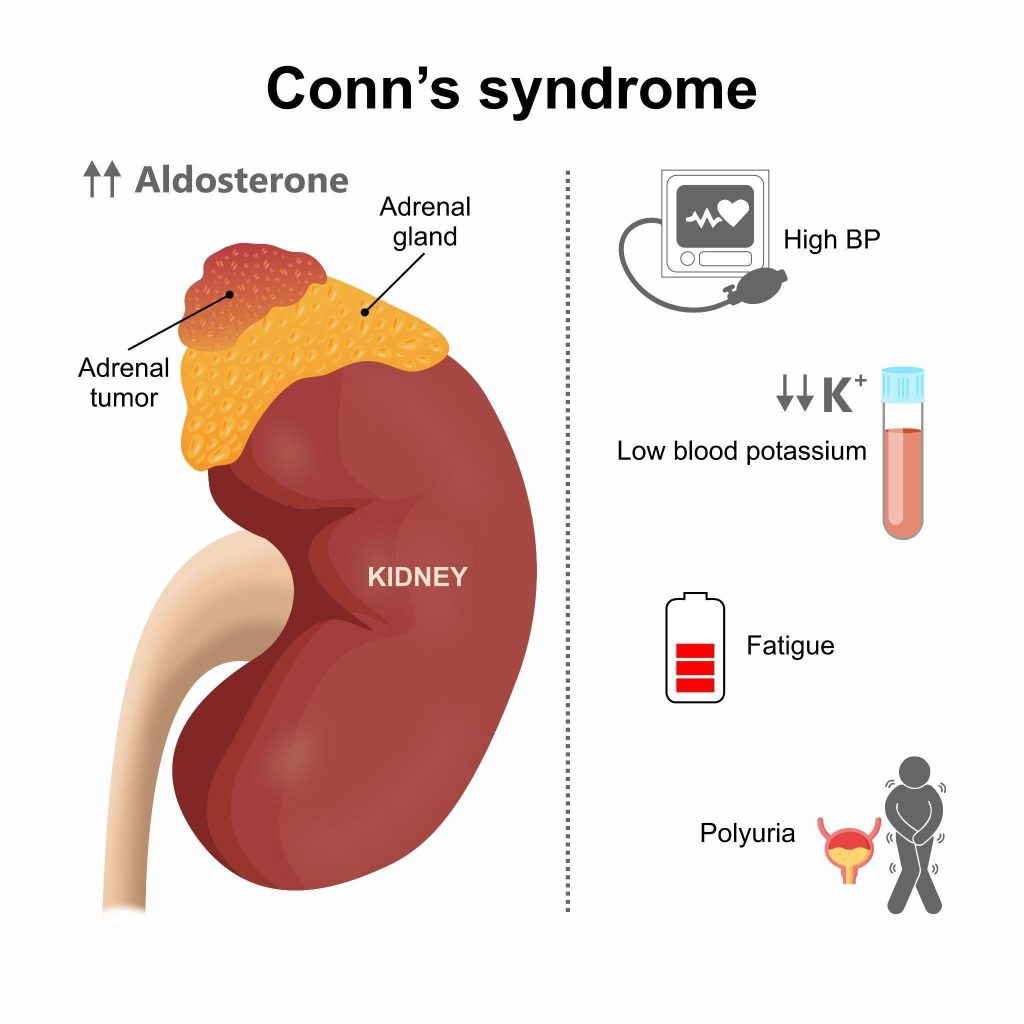
Aldosterone excess most commonly occurs in a condition known as primary hyperaldosteronism (Conn’s syndrome). In this disorder, one or both adrenal glands produce aldosterone independently of the body’s normal regulatory mechanisms.
Excess aldosterone leads to:
Increased sodium retention
Increased water retention
Suppression of renin
Excess potassium loss
Over time, this contributes to hypertension that may be resistant to standard blood pressure medications and can increase the risk of heart disease, stroke and kidney damage.
What causes aldosterone excess?
Aldosterone levels may rise when the adrenal glands produce the hormone in excess (termed Primary Hyperaldosteronism. Understanding the cause is essential for selecting the most effective treatment.
Unilateral adrenal adenoma —a benign (non-cancerous) tumour in one adrenal gland that produces aldosterone independently of the body’s normal regulatory system, leading to persistent hormone overproduction.
Rare genetic conditions — inherited disorders, such as familial hyperaldosteronism, that alter how the adrenal glands regulate aldosterone production and can lead to early or recurrent hormone excess.
Primary hyperaldosteronism (Conn’s syndrome) is a condition where the adrenal glands produce too much aldosterone, leading to high blood pressure and low potassium levels.
What are the symptoms of aldosterone excess?
Excess aldosterone affects blood pressure regulation and electrolyte balance. Symptoms often develop gradually and may go unnoticed until evaluation for persistent hypertension or abnormal potassium levels.
High blood pressure — persistent or difficult-to-control hypertension caused by increased sodium retention.
Low potassium levels — fatigue, cramps or muscle weakness due to excessive loss of potassium in the urine.
Muscle cramps or weakness — resulting from an electrolyte imbalance affecting normal muscle function.
Excessive thirst — increased fluid needs as the body attempts to correct the altered sodium balance.
Frequent urination — higher urine output linked to changes in kidney handling of sodium and potassium.
How is aldosterone excess diagnosed?
Diagnosis involves a combination of blood tests, imaging studies and clinical evaluation. These assessments help identify the source of the imbalance and guide appropriate treatment planning.
Aldosterone–renin ratio (ARR) — a blood test that compares aldosterone and renin levels. When aldosterone is elevated while renin is suppressed, the resulting high ratio raises suspicion for primary hyperaldosteronism.
Confirmatory testing — may include saline suppression testing or other hormone assessments to confirm inappropriate aldosterone production.
Electrolyte testing — measurement of potassium and sodium levels.
Adrenal imaging (CT scan) — identifies structural abnormalities such as adenomas. Done after confirmation of hyperaldosteronism.
Adrenal vein sampling (when required) — a specialised procedure used to determine whether excess aldosterone originates from one or both adrenal glands before surgery is considered.
Medication review is essential, as certain blood pressure drugs can affect renin and aldosterone levels.
What are the treatment options for aldosterone excess?
Treatment depends on the underlying cause, the severity of symptoms and findings on blood tests or imaging. Most cases respond well to medication, while some require targeted procedures or specialist care.
Potassium supplementation — correcting low potassium levels when required for safety and symptom relief.
Minimally invasive adrenal surgery — laparoscopic adrenalectomy may be recommended for confirmed unilateral aldosterone-producing adenomas. Surgery can significantly improve or even cure hypertension in selected patients.
Long-term monitoring — regular hormone testing, blood pressure checks and symptom review to ensure ongoing safety and effectiveness.
What to expect during aldosterone suppression
Treatment for aldosterone involves ongoing supervision to ensure hormone levels return to a safe range and symptoms improve steadily. Regular monitoring helps guide adjustments and prevents complications.
Regular blood pressure checks — tracking blood pressure to assess response to aldosterone-blocking treatment.
Repeat hormone testing — measuring aldosterone and renin levels periodically ensures treatment is suppressing excess hormone activity appropriately.
Electrolyte monitoring — checking potassium and sodium levels helps detect and prevent imbalances caused by the condition or its treatment.
Kidney function tests — assessing renal function ensures medications remain safe and do not adversely affect kidney health.
Medication dose adjustments — doses may be modified based on blood pressure response, laboratory results and overall clinical progress.
Potential benefits of curing Primary Hyperaldosteronism
Effective treatment of aldosterone excess can improve blood pressure control, restore electrolyte balance and reduce long-term cardiovascular risk. Outcomes depend on the underlying cause and how early the condition is identified.
Improved blood pressure control — blocking aldosterone reduces sodium and water retention, helping stabilise blood pressure, particularly in resistant hypertension.
Reduced reliance on multiple medications — targeted treatment may lower the number or dosage of antihypertensive drugs required over time.
Correction of potassium levels — restoring normal potassium improves muscle function, reduces cramps and prevents complications linked to chronic hypokalaemia.
Lower cardiovascular risk — treating aldosterone excess decreases strain on the heart and blood vessels, reducing the risk of stroke, heart enlargement and heart failure and bringing it back down to levels of the normal person.
Protection of kidney function — proper hormonal control helps prevent long-term kidney damage associated with uncontrolled hypertension.
Improved overall well-being — many patients experience better energy levels and physical comfort once blood pressure and electrolyte balance are stabilised.
Risks and precautions for aldosterone suppression
While treatment is generally safe, certain considerations apply.
Medication side effects — spironolactone may cause breast tenderness, menstrual irregularities or elevated potassium. Eplerenone has fewer hormonal side effects but may still affect potassium levels.
Kidney function considerations — reduced kidney function requires careful monitoring.
Risk of high potassium (hyperkalaemia) — particularly in patients with kidney disease or those on certain blood pressure medications.
Surgical risks — as with any procedure, adrenal surgery carries standard operative risks, though laparoscopic approaches are generally safe.
Specialist endocrine assessment ensures appropriate selection and safe management.
Summary
Aldosterone excess is a treatable hormonal condition that commonly presents as resistant hypertension and may be associated with low potassium levels. Primary hyperaldosteronism is one of the most underdiagnosed causes of secondary hypertension. Early detection through proper hormonal testing allows targeted treatment, which may include medication or minimally invasive surgery. With appropriate management and monitoring, blood pressure control improves and long-term cardiovascular risk can be significantly reduced.
If you have persistent high blood pressure, low potassium levels or hypertension that is difficult to control, schedule a consultation with The Metabolic Clinic for a comprehensive endocrine evaluation and personalised treatment plan.
Primary hyperaldosteronism is more common than previously thought and may account for 5–10% of hypertension cases, particularly resistant hypertension.
No. Many patients have normal potassium levels, especially in early stages.Though this is the number one marker that someone may have primary hyperaldosteronism.
Blood pressure often improves significantly. Some patients may still require reduced-dose medication expecially if they have had the condition for a long time thus causing permanent stiffening of arteries.
That depends on the cause. Bilateral adrenal overactivity typically requires long-term medication, while surgery may be definitive for unilateral disease.
Testing is recommended for individuals with resistant hypertension, high blood pressure at a young age, unexplained low potassium levels or an adrenal nodule detected on imaging.
No. Aldosterone excess involves abnormal mineralocorticoid production affecting blood pressure and potassium, while Cushing’s syndrome is caused by excess cortisol and presents with different hormonal features.
chat with us
Welcome to The Metabolic Clinic
Holistic Care for Hormones, Bones, and Metabolic Health
Dr Dinesh graduated with honours from Monash University, Melbourne in 2009, receiving the Prince Henry's Prize in Surgery. During his endocrinology training in Melbourne, he won the top registrar award at the Endocrine Society of Australia Clinical Weekend in 2016, followed by securing Australia's only Andrology fellowship in 2017. Upon returning to Singapore, he was the sub-speciality lead for adrenal, pituitary, and bone services at Khoo Teck Puat Hospital and established The Metabolic Bone Clinic.
A passionate educator, he served as Associate Programme Director for Endocrinology at NHG, training the next generation of endocrinologists, and received the NHG Teaching Award for Senior Doctors in 2023. An expert endocrinologist with proficiency in both general and sub-speciality endocrinology, he has an interest in longevity through improving cardiovascular risk, metabolism, bone health, and muscle loss prevention, with the ultimate aim of improving the number of healthy years in one's life.
10+ Years of Experience in Hormone & Metabolic Health
Founder of The Metabolic Bone Clinic in Khoo Teck Puat Hospital
Sub-specialist training with international experts in Melbourne, Australia
Clinical Interest in Longevity & Metabolic Health
START YOUR PERSONALISED HEALTH JOURNEY
If you’re not achieving your treatment targets, struggling with weight changes, fatigue, or unexplained symptoms—it’s time to take a deeper look.
Get clarity with a tailored plan built around you and improving your metabolic health.