Diabetic Nephropathy: When High Blood Sugar Damages the Kidneys
May 28, 2026
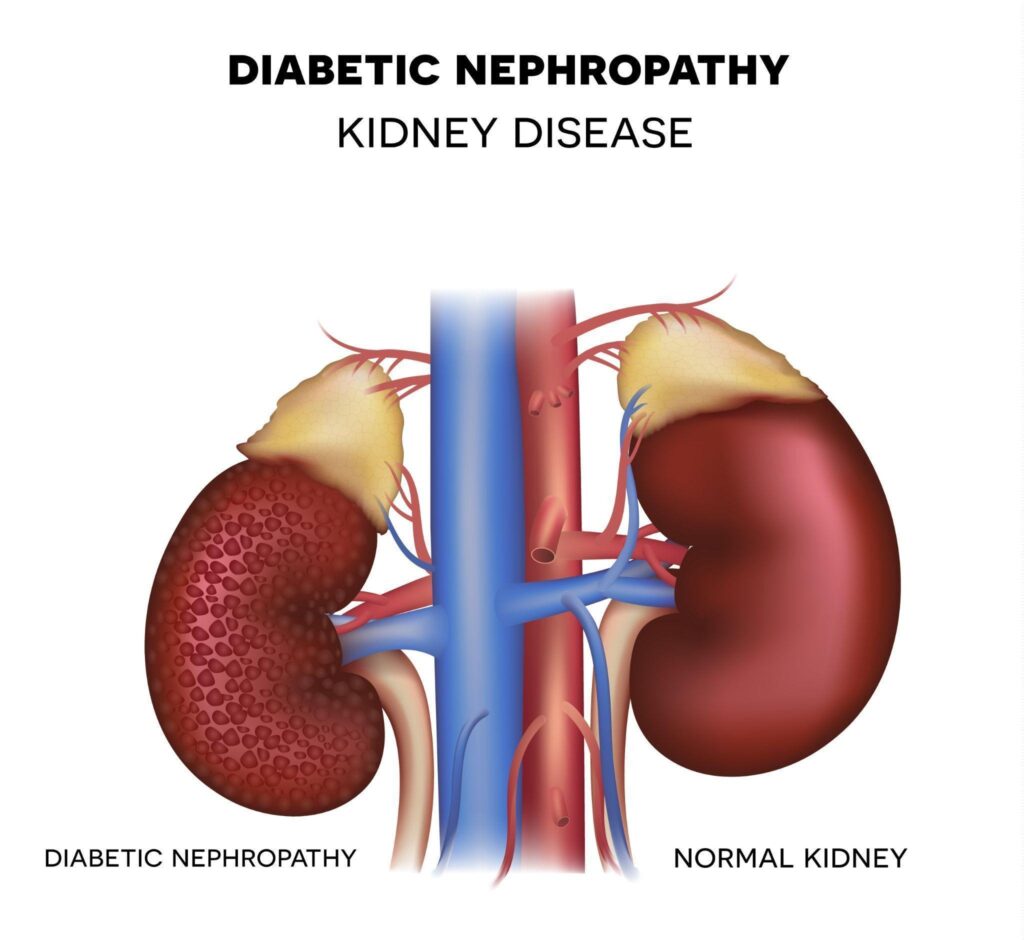
Diabetic nephropathy is a diabetes-related condition in which prolonged high blood sugar damages the kidneys’ filtering function over time.
Diabetic nephropathy is one of the most significant long-term complications of diabetes, yet it often develops without clear warning in its early stages. Persistently high blood sugar places ongoing stress on the small blood vessels within the kidneys, gradually affecting their ability to filter waste and maintain the body’s internal balance. This process unfolds slowly, and for many individuals, it begins long before any symptoms become apparent.
Because early kidney damage does not usually cause pain or noticeable changes, it is frequently detected only through routine screening instead of clinical symptoms. As the condition progresses, signs such as swelling, fatigue or changes in urination may start to appear, reflecting a decline in kidney function.
What is diabetic nephropathy and how does it affect the kidneys?
The kidneys play a vital role in keeping the body in balance. They filter waste products and excess fluid from the blood, regulate electrolytes and help control blood pressure. This work is carried out by millions of tiny filtering units called glomeruli, which act as fine sieves, allowing waste to pass into the urine while retaining essential proteins and cells in the bloodstream [1].
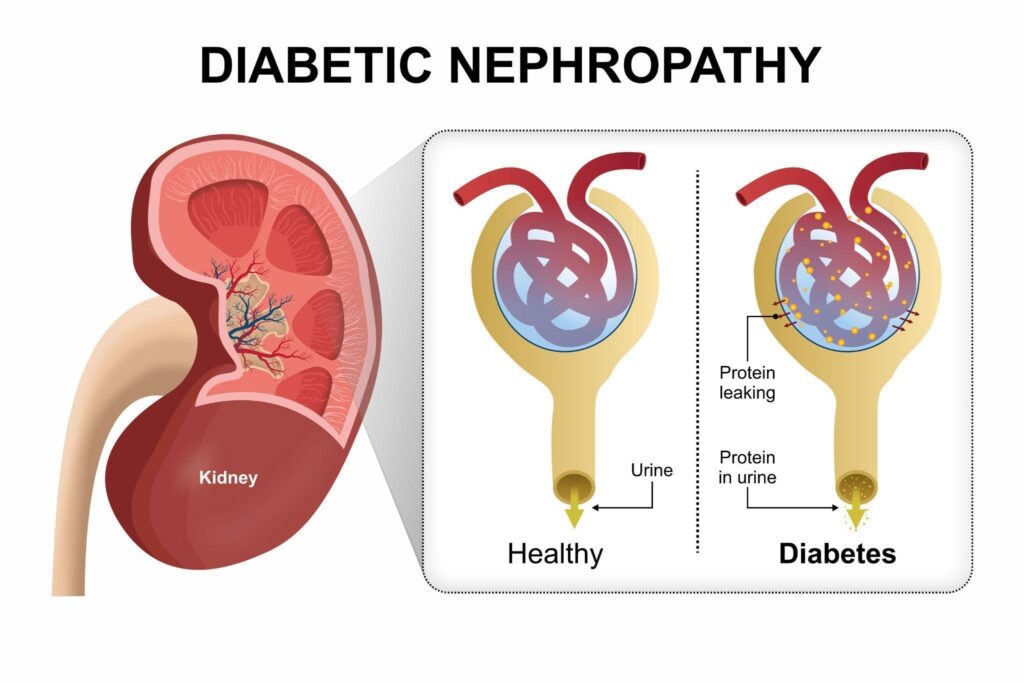
Diabetic nephropathy develops when persistently high blood sugar begins to affect these delicate structures [2]. Over time, elevated glucose levels damage the small blood vessels within the glomeruli, making them less efficient and more permeable than they should be. As a result, important proteins, particularly albumin, start to leak into the urine, a change that is often one of the earliest detectable signs of kidney involvement in diabetes [3]. A urine albumin check is essential in diabetes monitoring for this reason.
As this damage progresses, the kidneys gradually lose their ability to filter waste effectively. Waste products can begin to build up in the blood, and the body’s fluid balance may be disrupted. Without timely management, this can lead to a steady decline in kidney function, increasing the risk of chronic kidney disease and, in advanced cases, kidney failure.
Diabetic nephropathy damages the kidney’s filtering units, causing them to leak protein into the urine and gradually lose their ability to filter waste effectively.
How does high blood sugar damage the kidneys over time?
High blood sugar does not damage the kidneys all at once. The effect builds gradually, as sustained glucose levels begin to alter how the kidneys function at a microscopic level. Over time, this ongoing strain disrupts normal filtration and places pressure on the kidney’s delicate structures, leading to progressive changes that can affect overall kidney health [4].
Damage to small blood vessels — Prolonged high glucose levels weaken and injure the tiny blood vessels in the kidneys, affecting their ability to function properly.
Increased pressure within the kidneys — The kidneys are forced to work harder, creating internal pressure that accelerates structural damage over time.
Protein leakage into urine (albuminuria) — The filtering system becomes less selective, allowing proteins such as albumin to pass into the urine, often an early warning sign.
Gradual decline in kidney function — As damage accumulates, the kidneys become less effective at filtering waste, leading to a slow reduction in function.
What are the early signs of diabetic kidney disease?
Diabetic kidney disease often develops quietly, especially in the early stages. Changes tend to begin at a microscopic level, which means there may be no obvious symptoms initially. This is why routine screening plays an important role in identifying early signs before noticeable complications arise.
Often no symptoms in the early stages — Kidney damage can be present without any visible or physical signs, until it becomes ‘end-stage’ (too late to reverse).
Microalbuminuria — Small amounts of protein (albumin) appear in the urine, usually detected through laboratory testing rather than symptoms.
Mild swelling in the hands or feet — Fluid retention may develop as kidney function begins to change [5].
Subtle fatigue — A general sense of tiredness may occur as the body’s ability to filter waste becomes less efficient.
Diabetic nephropathy may cause mild swelling in the hands or feet due to fluid retention as kidney function begins to decline.
What are the stages of diabetic nephropathy?
Diabetic nephropathy progresses through several stages, with each stage reflecting increasing levels of kidney involvement and declining function. Doctor’s will classify this differently and it will be based on EGFR (kidney blood test) as well as protein leakage (Using something called the KDIGO guidelines) but the unofficial stages below serve as a way to understand worsening kidney function and what happens.
Early stage (microalbuminuria) — At this stage, small amounts of albumin begin to leak into the urine, usually detected only through laboratory testing [6]. There are typically no symptoms, and kidney function remains largely preserved. This stage is clinically important because timely intervention can help slow or even halt further progression.
Moderate stage (macroalbuminuria) — Protein leakage becomes more pronounced, indicating more established damage to the kidney’s filtering system [7]. Some individuals may begin to develop mild swelling or changes in blood pressure. Without appropriate management, kidney function may start to decline more noticeably during this phase.
Advanced stage (chronic kidney disease) — The kidneys lose a significant portion of their filtering capacity [8]. Waste products and excess fluid begin to accumulate in the body, which may lead to symptoms such as fatigue, swelling, and reduced appetite. Medical management becomes more intensive at this stage to preserve remaining kidney function.
End-stage kidney disease — Kidney function falls to a level where the kidneys can no longer adequately support the body’s needs. At this point, renal replacement therapy, such as dialysis or kidney transplantation, is required to maintain life.
Why is diabetic nephropathy often diagnosed late?
Diabetic nephropathy is often diagnosed at a later stage because its early course does not usually produce noticeable symptoms. The initial changes in kidney function develop gradually and remain clinically silent, which means there is little to prompt concern or medical evaluation based on how a person feels.
Another contributing factor is the absence of routine screening. Early indicators, such as small amounts of protein in the urine, can only be detected through specific tests. Without regular monitoring, these changes may go unnoticed for years, particularly in individuals who do not undergo consistent follow-up for diabetes.
By the time symptoms begin to appear, the condition has often progressed. Signs such as swelling, fatigue or changes in urination tend to reflect more advanced involvement, when kidney function has already been affected.
When should you see an endocrinologist in Singapore?
It is important to seek specialist care when there are concerns about diabetes control or possible kidney involvement. An endocrinologist can carry out a detailed assessment, review your current treatment and monitor for early complications that may not yet be clinically obvious.
Persistent difficulty in controlling blood sugar levels, even with medication, is one of the most common reasons for referral. Abnormal findings on urine or blood tests, such as protein in the urine or a reduced eGFR, also require further evaluation. In addition, symptoms like swelling or unexplained fatigue may reflect changes in kidney function. Individuals with long-standing diabetes benefit from regular specialist review, as the risk of complications increases over time.
How is diabetic nephropathy diagnosed?
Diabetic nephropathy is usually identified through a combination of laboratory tests and clinical assessment, often before symptoms become apparent. These tests help detect early changes in kidney function and monitor progression over time.
Urine albumin-to-creatinine ratio (ACR) — This test measures the amount of albumin in the urine relative to creatinine, providing a reliable indicator of abnormal protein leakage [9]. It is commonly used for routine screening, as even small increases can signal early kidney involvement before any symptoms develop.
Blood tests (creatinine, eGFR) — Blood creatinine levels are used to calculate the estimated glomerular filtration rate (eGFR), which reflects how efficiently the kidneys are filtering waste [10]. A declining eGFR indicates reduced kidney function and helps determine the stage and progression of the condition.
Blood pressure monitoring — Blood pressure is closely linked to kidney health, and elevated levels can both worsen kidney damage and result from it. Regular monitoring helps guide treatment decisions and is an essential part of managing diabetic nephropathy.
Can diabetic nephropathy be reversed or slowed down?
Diabetic nephropathy is not usually reversible once structural damage to the kidneys has developed. However, the course of the condition is not fixed, and progression/deterioration can often be slowed with timely and consistent management. Identifying changes at an early stage is particularly important, as intervention at this point can help preserve kidney function and delay further deterioration.
Strict blood sugar control remains central to this approach, as persistently elevated glucose levels continue to drive kidney damage. Alongside this, regular monitoring and appropriate medical care allow for adjustments in treatment based on how the condition is evolving. With a structured and proactive approach, many individuals are able to maintain stable kidney function for extended periods and reduce the likelihood of progression to advanced stages.
What treatments help protect kidney function?
Protecting kidney function in diabetic nephropathy requires a combination of medical treatment and ongoing disease management. The aim is to reduce stress on the kidneys, control contributing factors and slow further decline.
Blood sugar management — Maintaining stable glucose levels helps reduce ongoing damage to the kidneys and is a key component of long-term control.
Blood pressure control — Keeping blood pressure within target range reduces strain on the kidneys and lowers the risk of progression.
Cholesterol management — Controlling cholesterol levels supports overall vascular health and reduces additional risk to the kidneys.
Medications (ACE inhibitors, ARBs, SGLT2 inhibitors, Nonsteroidal Mineralocorticoid Antagonists, GLP-1 Agonists) — Medications now play a major role in protecting kidney function in people with diabetic nephropathy. Alongside blood sugar and blood pressure control, several newer medication groups have been shown to slow kidney damage, reduce protein leakage in the urine and lower the risk of progression to kidney failure [11]. In many patients, a combination of medications may be used as part of long-term kidney protection and cardiovascular risk reduction.
ACE Inhibitors and ARBs — ACE inhibitors and angiotensin receptor blockers (ARBs) are commonly used to control blood pressure and reduce pressure within the kidneys [12]. They help lower protein leakage in the urine and slow the progression of diabetic kidney disease. These medications are often recommended even in the earlier stages of diabetic nephropathy when protein in the urine is detected [13].
SGLT2 Inhibitors — SGLT2 inhibitors have become an important part of diabetic kidney disease management due to their significant kidney-protective benefits [14]. These medications help reduce excess glucose reabsorption in the kidneys and lower pressure within the filtering units of the kidneys. Studies have shown that SGLT2 inhibitors can slow decline in kidney function, reduce the risk of kidney failure and delay the need for dialysis in suitable patients [15]. This medication is fast becoming first-line especially in the context of kidney disease and can even improve kidney disease in patients without diabetes.
GLP-1 Receptor Agonists — GLP-1 receptor agonists help improve blood sugar control and may also provide cardiovascular and kidney benefits. In patients with type 2 diabetes and diabetic nephropathy, these medications help reduce progression of kidney disease while supporting weight management and metabolic health [16].
Non-Steroidal Mineralocorticoid Receptor Antagonists (Finerenone) — Non-steroidal mineralocorticoid receptor antagonists such as finerenone may help reduce inflammation and scarring within the kidneys [17]. They are used in selected patients with diabetic kidney disease to further reduce the risk of kidney function decline and cardiovascular complications, particularly when kidney damage continues despite standard treatment.
What lifestyle changes can help protect your kidneys?
Lifestyle measures play an important role in supporting kidney health alongside medical treatment. Consistent, well-managed habits can reduce the overall burden on the kidneys and help stabilise blood sugar and blood pressure over time.
Diet (reduced salt, balanced nutrition) — Limiting salt intake helps control blood pressure, which is closely linked to kidney health. A balanced diet that supports stable blood sugar levels can reduce ongoing stress on the kidneys and improve overall metabolic control.
Regular exercise — Physical activity improves insulin sensitivity and helps maintain better glucose control. It also supports cardiovascular health, which is important because the kidneys rely on healthy blood vessels to function effectively.
Weight management — Maintaining a healthy weight reduces the metabolic demand on the body and lowers the risk of worsening insulin resistance. This, in turn, helps reduce the progression of kidney-related complications.
Avoiding smoking — Smoking damages blood vessels and can accelerate the decline in kidney function. Avoiding tobacco use helps preserve circulation and slows the progression of kidney disease.
What happens If diabetic nephropathy is left untreated?
Without appropriate management, diabetic nephropathy tends to progress over time, leading to a gradual but continuous decline in kidney function. The damage to the kidney’s filtering system does not stabilise on its own, and ongoing exposure to high blood sugar and associated factors continues to worsen the condition.
As kidney function declines, the body becomes less effective at removing waste products and excess fluid. This can result in the development of chronic kidney disease, where waste begins to accumulate in the bloodstream and affects overall health. Individuals may start to experience symptoms such as fatigue, swelling and reduced appetite as the condition advances.
In the later stages, kidney function may fall to a level where the kidneys can no longer support the body’s needs. At this point, renal replacement therapy becomes necessary. This may involve dialysis to filter the blood or, in suitable cases, a kidney transplant to restore function.
Summary
Diabetic nephropathy is a progressive complication of diabetes that develops when persistently high blood sugar begins to affect the kidneys over time. The condition often starts without noticeable symptoms, which makes early detection through routine screening especially important.
As the disease progresses, subtle changes such as protein in the urine may appear first, followed by a gradual decline in kidney function. If not identified and managed early, this can lead to chronic kidney disease and, in advanced cases, the need for dialysis or transplantation.
A clear understanding of how diabetic nephropathy develops highlights the importance of consistent management. Regular monitoring, good blood sugar control, appropriate medications and supportive lifestyle measures all play a role in slowing progression and protecting kidney function. With timely intervention, many individuals can maintain stable kidney health and reduce the risk of serious complications.
If you have diabetes or concerns about your kidney health, schedule a consultation with The Metabolic Clinic for a personalised assessment and early management plan. With appropriate lifestyle and medication changes, kidney deterioration can be halted.
Samsu, N. (2021). Diabetic nephropathy: Challenges in pathogenesis, diagnosis, and treatment. BioMed Research International, 2021, 1497449. https://doi.org/10.1155/2021/1497449
Zelmanovitz, T., Gerchman, F., Balthazar, A. P., Thomazelli, F. C., Matos, J. D., & Canani, L. H. (2009). Diabetic nephropathy. Diabetology and Metabolic Syndrome, 1, 10. https://doi.org/10.1186/1758-5996-1-10
Chida, S., Fujita, Y., Ogawa, A., Hayashi, A., Ichikawa, R., Kamata, Y., Takeuchi, A., Takano, K., & Shichiri, M. (2016). Levels of albuminuria and risk of developing macroalbuminuria in type 2 diabetes: Historical cohort study. Scientific Reports, 6, 26380. https://doi.org/10.1038/srep26380
Selby, N. M., & Taal, M. W. (2020). An updated overview of diabetic nephropathy: Diagnosis, prognosis, treatment goals and latest guidelines. Diabetes, Obesity & Metabolism, 22 Suppl 1, 3–15. https://doi.org/10.1111/dom.14007
Huan, L., Yuezhong, L., Chao, W., & HaiTao, T. (2016). The urine albumin-to-creatinine ratio is a reliable indicator for evaluating complications of chronic kidney disease and progression in IgA nephropathy in China. Clinics, 71(5), 243–250. https://doi.org/10.6061/clinics/2016(05)01
Davis, K. N., Hines, A. E., Schaefer, M. C., & Naseman, K. W. (2022). Protecting the kidneys: Update on therapies to treat diabetic nephropathy. Clinical Diabetes : A Publication of the American Diabetes Association, 40(3), 305–311. https://doi.org/10.2337/cd21-0090
Avula, A., Johal, L. K., Ali, F., Amir, S., Yadav, S., Murtuza, M., Zia, U., Janjua, F. F., Raza, A., Lal, K., Abid, M., & Khan, R. (n.d.). Ace inhibitors and arbs in chronic kidney disease: A systematic review of randomized controlled trials on albuminuria reduction, egfr decline, and safety. Cureus, 17(10), e93707. https://doi.org/10.7759/cureus.93707
Vivian, E., & Mannebach, C. (2013). Therapeutic approaches to slowing the progression of diabetic nephropathy – is less best? Drugs in Context, 2013, 212249. https://doi.org/10.7573/dic.212249
Padda, I. S., Mahtani, A. U., & Parmar, M. (2026). Sodium-glucose transport 2 (Sglt2) inhibitors. In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK576405/
Yau, K., Dharia, A., Alrowiyti, I., & Cherney, D. Z. I. (2022). Prescribing sglt2 inhibitors in patients with ckd: Expanding indications and practical considerations. Kidney International Reports, 7(7), 1463–1476. https://doi.org/10.1016/j.ekir.2022.04.094
Yu, J. H., Park, S. Y., Lee, D. Y., Kim, N. H., & Seo, J. A. (2022). GLP-1 receptor agonists in diabetic kidney disease: Current evidence and future directions. Kidney Research and Clinical Practice, 41(2), 136–149. https://doi.org/10.23876/j.krcp.22.001
Kolkhof, P., Lawatscheck, R., Filippatos, G., & Bakris, G. L. (2022). Nonsteroidal mineralocorticoid receptor antagonism by finerenone—Translational aspects and clinical perspectives across multiple organ systems. International Journal of Molecular Sciences, 23(16), 9243. https://doi.org/10.3390/ijms23169243
chat with us
Welcome to The Metabolic Clinic
Holistic Care for Hormones, Bones, and Metabolic Health
Dr Dinesh graduated with honours from Monash University, Melbourne in 2009, receiving the Prince Henry's Prize in Surgery. During his endocrinology training in Melbourne, he won the top registrar award at the Endocrine Society of Australia Clinical Weekend in 2016, followed by securing Australia's only Andrology fellowship in 2017. Upon returning to Singapore, he was the sub-speciality lead for adrenal, pituitary, and bone services at Khoo Teck Puat Hospital and established The Metabolic Bone Clinic.
A passionate educator, he served as Associate Programme Director for Endocrinology at NHG, training the next generation of endocrinologists, and received the NHG Teaching Award for Senior Doctors in 2023. An expert endocrinologist with proficiency in both general and sub-speciality endocrinology, he has an interest in longevity through improving cardiovascular risk, metabolism, bone health, and muscle loss prevention, with the ultimate aim of improving the number of healthy years in one's life.
10+ Years of Experience in Hormone & Metabolic Health
Founder of The Metabolic Bone Clinic in Khoo Teck Puat Hospital
Sub-specialist training with international experts in Melbourne, Australia
Clinical Interest in Longevity & Metabolic Health
START YOUR PERSONALISED HEALTH JOURNEY
If you’re not achieving your treatment targets, struggling with weight changes, fatigue, or unexplained symptoms—it’s time to take a deeper look.
Get clarity with a tailored plan built around you and improving your metabolic health.