Being diagnosed with thyroid cancer can feel overwhelming. But it is important to know that most cases are highly treatable, especially when detected early.
In Singapore, thyroid cancer is one of the top 10 cancers among women. It affects individuals of all ages and sex but is most frequently diagnosed in women between 30, and 60 years old with females having a four times higher risk. Fortunately, many types of thyroid cancer grow slowly, and respond well to treatment, especially when detected early. Thus the prognosis is favourable.
While thyroid cancer can be a daunting diagnosis, advances in diagnosis, and treatment have significantly improved patient outcomes. With timely intervention, and personalised care, many individuals go on to lead healthy, full lives.
Types of Thyroid Cancer
Thyroid cancer is not a single disease but a group of cancers that arise from different types of cells within the thyroid gland. The most common types originate from follicular cells, which are responsible for producing thyroid hormones. Each type varies in how aggressive it is, how it spreads, and how it is treated, as per the table below:
TYPE
CELL OF ORIGIN
COMMON FEATURES
SPREAD PATTERN
PROGNOSIS
Papillary Thyroid Carcinoma (PTC)
Follicular cells
Most common type.Often affects young to middle-aged adults.May present with lymph node swelling.
Spreads via lymphatic system (neck lymph nodes).
Excellent, especially in the early stages.
Follicular Thyroid Carcinoma (FTC)
Follicular cells
Slightly older age group.Less likely to involve lymph nodes.May invade blood vessels.
Tends to spread through bloodstream (lungs, bones).
Good, but lower than PTC.
Hurthle Cell Carcinoma
Variant of follicular cells (Hurthle cells)
More aggressive.Higher risk of recurrence.Less responsive to radioactive iodine.
May spread locally, and distantly.
Fair, depends on stage.
Medullary Thyroid Carcinoma (MTC)
Parafollicular C-cells
Multiple Endocrine Neoplasia type 2 (MEN2).Associated with elevated calcitonin levels.Requires genetic screening.Rare
Spreads to lymph nodes, and distant organs.
Variable, but better if localised.
Anaplastic Thyroid Carcinoma (ATC)
Undifferentiated follicular cells
Rare but very aggressive.Rapid growth.Often presents with neck compression symptoms.
Rapid local invasion, and distant spread.
Poor (often advanced at diagnosis) with rapid deterioration.
What causes Thyroid Cancer?
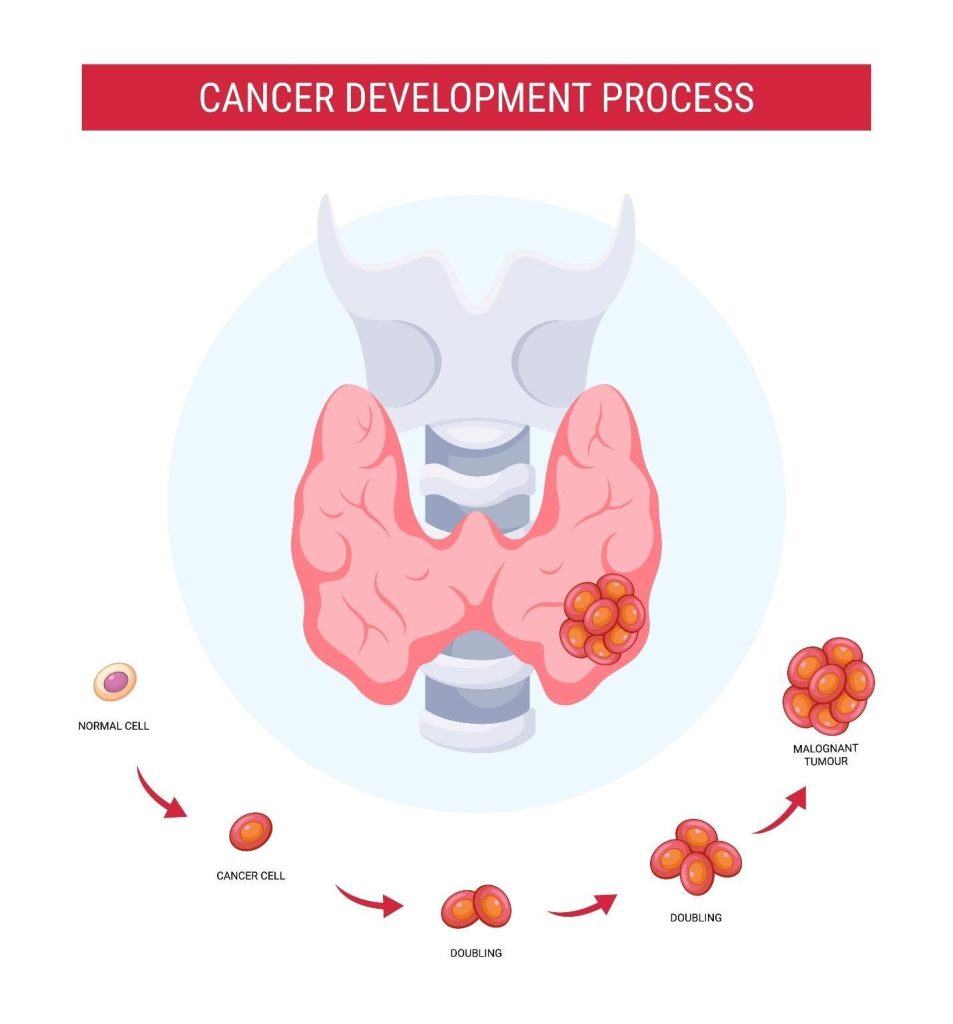
The exact cause of thyroid cancer is not always clear. However, a number of factors are known to increase your risk by triggering changes (mutations) in the DNA of thyroid cells. These mutations affect how cells grow, divide, and die, and may cause uncontrolled cell growth, leading to the formation of a cancerous tumour.
These risk factors include:
CAUSES
HOW IT TRIGGERS THYROID CANCER
Genetic mutations (both inherited and acquired)
Thyroid cancer often begins at the molecular level, where genetic mutations alter the behaviour of normal thyroid cells. These mutations can be:Inherited (germline mutations) passed down through families, such as in familial medullary thyroid cancer.Acquired (somatic mutations) that develop over a person’s lifetime due to environmental exposures or unknown factors. Some common mutations seen in thyroid cancer include:RET proto-oncogene mutations (especially in medullary thyroid cancer).BRAF, and RAS mutations (common in papillary thyroid cancer).
Family history of thyroid cancer or genetic syndromes
Having a first-degree relative (such as a parent or sibling) with thyroid cancer significantly raises your risk. Sometimes, thyroid cancer is part of a hereditary cancer syndrome, such as: Multiple Endocrine Neoplasia type 2 (MEN2)– associated with mutations in the RET gene. Familial medullary thyroid carcinoma (FMTC)– a non-syndromic inherited form of thyroid cancer. These syndromes predispose individuals to develop thyroid cancer, often at a younger age and in more aggressive forms.
Existing thyroid conditions, such as multinodular goitre or Hashimoto’s thyroiditis
Having certain pre-existing thyroid disorders may increase your risk:Multinodular goitre results in multiple nodules forming within the thyroid. While most are benign, the presence of multiple abnormal growths can increase the chance of one becoming malignant. Hashimoto’s thyroiditis is an autoimmune condition that causes chronic inflammation of the thyroid gland. This ongoing inflammation can lead to cellular damage, and abnormal repair processes, increasing the risk of thyroid lymphoma or papillary thyroid cancer.
Iodine deficiency or excess
The thyroid relies on iodine to produce hormones. Both too little, and too much iodine can disrupt thyroid function and cell growth: Iodine deficiency can lead to goitre, and stimulate abnormal cell proliferation. Excess iodine, meanwhile, may trigger inflammation or oxidative stress in thyroid cells. These imbalances may contribute to the development of thyroid nodules, some of which carry the risk of becoming cancerous over time.
Radiation exposure during childhood
Radiation exposure, particularly to the head, neck or chest area during childhood, is one of the most well-established risk factors for thyroid cancer. Sources of radiation may include: Past radiation therapy for conditions like acne, enlarged tonsil, or lymphoma. Environmental exposure from nuclear accidents. Radiation damages the DNA within thyroid cells, increasing the risk of mutations that lead to cancer. The thyroid gland is especially sensitive to radiation in children, which explains why those exposed early in life have a higher risk.
Can Thyroid Nodules progress to Thyroid Cancer?
Thyroid nodules are common growths or lumps that form within the thyroid gland. These nodules are non-cancerous, and do not pose a serious health risk.
How does this happen?
The progression from a benign thyroid cell to thyroid cancer is usually driven by genetic mutations, and abnormal cell growth. Over time, certain mutations may cause the cell to divide uncontrollably, leading to the formation of a malignant tumour.
Some of the factors that may increase the likelihood of a thyroid nodule becoming cancerous include:
Family history of thyroid cancer or hereditary syndromes.
Presence of suspicious features on ultrasound, such as irregular shape, microcalcifications or increased blood flow.
Radiation exposure to the head or neck, especially during childhood.
Rapid growth of the nodule or associated symptoms like hoarseness or difficulty swallowing.
While most thyroid nodules are benign, a small percentage may turn cancerous over time.
Monitoring Is Key
Most benign thyroid nodules remain harmless, but it is essential to monitor them through:
Regular ultrasound scans to assess changes in size or structure.
Fine-needle aspiration biopsy (FNAB) to evaluate suspicious nodules.
Thyroid function tests to determine if the nodule affects hormone levels.
In fact, early detection of changes in a thyroid nodule can help identify cancer at its earliest stage, when treatment is most effective.
Symptoms of Thyroid Cancer
A recently found, persistent lump in the neck may be one of the earliest warning signs of thyroid cancer.
Thyroid cancer is often silent in its early stages, but as it progresses, the following symptoms may appear:
A painless lump or swelling in the neck.
Hoarseness or voice changes.
Difficulty swallowing or breathing.
Persistent cough not linked to a cold.
Neck or throat pain, sometimes radiating to the ears.
Swollen lymph nodes in the neck.
Who is at risk of Thyroid Cancer?
Several factors may increase your risk of developing thyroid cancer, including:
Age– thyroid cancer can occur at any age, but it is most diagnosed in people between 30, and 60 years old. The risk may be related to cumulative DNA damage.
Gender– females are more likely to develop thyroid cancer than males, particularly papillary thyroid carcinoma. This may be due to the influence of reproductive hormones, especially oestrogen, on thyroid tissue growth, and function.
Family history– individuals with a first-degree relative (parent, sibling, or child) who has had thyroid cancer are at higher risk. This may be due to inherited genetic mutations, shared environmental exposures or both.
Genetic conditions– some rare inherited syndromes, such as familial medullary thyroid cancer, and MEN2, significantly increase the risk of developing thyroid cancer, often at a younger age.
Medical history– a history of benign thyroid nodules, goitre or thyroid inflammation may increase the likelihood of malignant changes within the thyroid gland. Individuals with metabolic conditions like insulin resistance may also have a slightly increased risk.
Iodine imbalance– both iodine deficiency, and excess can affect thyroid function, and structure. Iodine deficiency may stimulate thyroid cell proliferation, while excess iodine can cause oxidative stress or inflammation, both of which may contribute to cancer risk. This is rare in Singapore where almost no one has iodine deficiency due to iodine supplementation in foods.
Radiation exposure–exposure to radiation in childhood, especially directed to the head, neck or chest, significantly increases the risk of thyroid cancer. This includes medical radiation therapy or accidental exposure. This is a strong risk factor.
Pre-existing thyroid nodules– while most thyroid nodules are benign, some may become cancerous, particularly if they are growing, firm, irregular or show suspicious features on ultrasound. This is only thought to affect 1 percent of benign nodules.
How is Thyroid Cancer diagnosed in Singapore?
Ultrasound imaging helps detect thyroid nodules, and assess their risk.
At The Metabolic Clinic, our endocrinologists use a comprehensive, and targeted approach to accurately diagnose thyroid cancer. This involves a combination of clinical assessment, advanced imaging, and specialised blood tests.
Physical Examination and Clinical Evaluation
Our evaluation begins with a detailed consultation, and physical examination:
Neck examination– our endocrinologist will palpate (feel) the thyroid gland, and surrounding areas for lumps, asymmetry or swollen lymph nodes.
Symptom review– symptoms such as a persistent hoarse voice, difficulty swallowing or a sensation of fullness in the neck are carefully assessed.
Medical and family history– a history of thyroid conditions, prior radiation exposure or familial syndromes like MEN2 can provide critical diagnostic clues.
Imaging Studies
We use imaging tests to examine the thyroid gland in detail, and assess any suspicious nodules or tumour spread:
Neck ultrasound– this is the first-line imaging test to visualise the structure of the thyroid, and nearby lymph nodes. It helps detect suspicious features such as irregular borders, microcalcifications or increased blood flow.
Fine-needle aspiration cytology (FNAC)– if a nodule appears suspicious, a biopsy is performed using a thin needle to extract cells for microscopic examination. FNAC is the standard for diagnosing thyroid cancer.
Computed Tomography (CT) or Magnetic Resonance Imaging (MRI) scan– these scans are used in selected cases to evaluate the extent of large or invasive tumours, and to assess involvement of surrounding structures, such as the trachea or blood vessels.
Radioactive iodine scan– this scan helps assess how well the thyroid gland absorbs iodine, which may indicate the presence or absence of functioning (hot) nodules versus non-functioning (cold) ones, which are more likely to be malignant.
Laboratory Testing
Blood tests play an important role in both diagnosis, and follow-up care:
Thyroid function tests– these include thyroid-stimulating hormone (TSH), T3, and T4 to assess whether the thyroid is underactive, overactive or functioning normally. Most thyroid cancers do not affect hormone levels, but testing helps rule out other thyroid conditions.
Calcitonin and carcinoembryonic antigen (CEA)– these tumour markers are particularly important in detecting and monitoring medullary thyroid cancer, which arises from C-cells.
Thyroglobulin– a protein produced by thyroid tissue, thyroglobulin is used as a tumour marker in papillary, and follicular thyroid cancers, after surgery to monitor for recurrence.
How is Thyroid Cancer treated in Singapore?
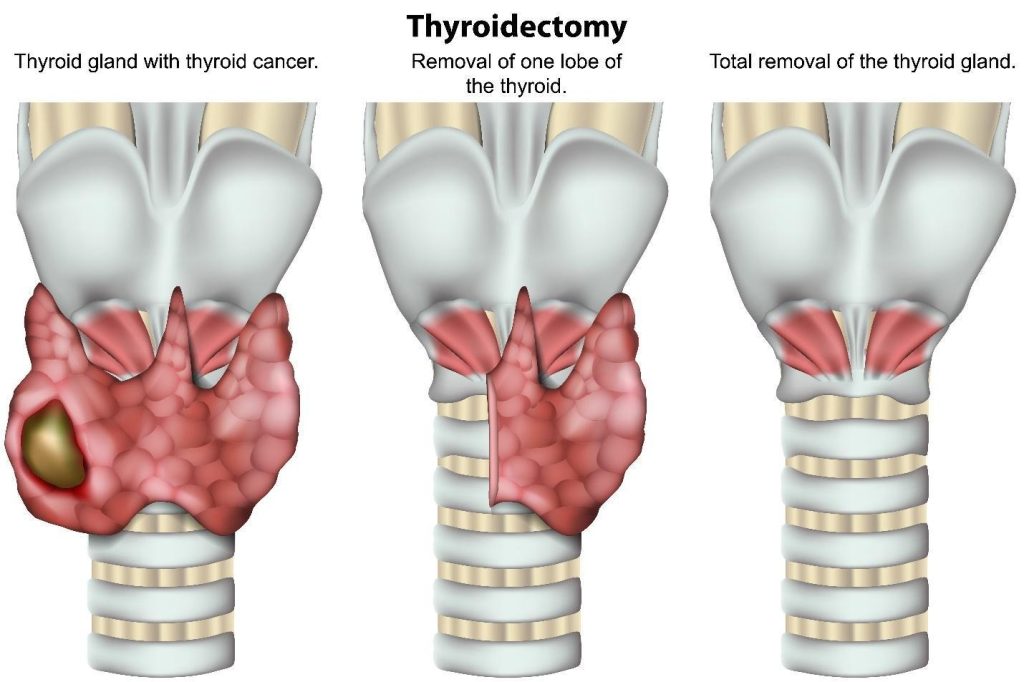
Surgery remains the mainstay of thyroid cancer treatment.
Treatment for thyroid cancer is highly individualised. It depends on several factors, including the type, and stage of the cancer, the patient’s age, overall health, and whether the cancer has spread beyond the thyroid gland.
Surgical Treatment
Surgery is often the first-line treatment for most types of thyroid cancer. Where surgical intervention is indicated, a referral will be made to a relevant surgical specialist for further evaluation and treatment.
Lymph node dissection– if the cancer has spread to nearby lymph nodes in the neck, these may also be surgically removed to reduce the risk of recurrence, and guide further treatment.
Thyroidectomy– this involves removing part (lobectomy) or all (total thyroidectomy) of the thyroid gland. A lobectomy may be sufficient for smaller, localised cancers, while total thyroidectomy is typically recommended for larger or more widespread tumours.
Radioactive Iodine (RAI) Therapy
Radioactive iodine therapy is commonly used after thyroidectomy, especially for papillary, and follicular thyroid cancers if deemed higher risk:
RAI is given orally in the form of a capsule or liquid.
It selectively destroys any remaining thyroid tissue or microscopic cancer cells, while sparing most other tissues in the body.
This therapy also helps with long-term surveillance, as it allows thyroglobulin levels to be used more reliably as a tumour marker.
TSH Suppressive Therapy
After surgery, patients usually require lifelong thyroid hormone replacement:
Levothyroxine is prescribed to replace the hormones normally produced by the thyroid gland in a higher dose than normal.
It also suppresses TSH, which could otherwise stimulate the growth of any remaining cancer cells.
External Beam Radiation Therapy
This treatment uses high-energy X-rays to target, and destroy cancer cells:
It is typically reserved for more aggressive, non-responsive or inoperable tumours, such as anaplastic thyroid cancer which cannot be treated by radioactive iodine.
It may also be used if cancer has spread beyond the thyroid, and cannot be fully removed by surgery.
Targeted Therapy and Chemotherapy
For advanced or treatment-resistant thyroid cancers, such as metastatic medullary or anaplastic thyroid cancers, systemic therapies may be considered:
Chemotherapy– less commonly used for most thyroid cancers, but may play a role in managing aggressive or rapidly progressing cancers that do not respond to other treatments.
Targeted therapy– these drugs block specific pathways or genetic mutations that cancer cells use to grow and divide (RET inhibitors or tyrosine kinase inhibitors).
Summary
Early diagnosis, and personalised care are key to successful thyroid cancer treatment.
Being diagnosed with thyroid cancer can feel overwhelming. But it is important to know that most cases are highly treatable, especially when detected early. Many individuals go on to lead full, healthy lives after treatment, with regular monitoring and support. In fact, advancements in medical care mean that effective treatments are available and outcomes are often very positive.
If you have noticed a lump in your neck, changes in your voice or other persistent symptoms, please do not ignore them. Remember, early action can make all the difference. Schedule an appointment with us today for a thorough evaluation. Your health and peace of mind are our top priorities.
No, most thyroid nodules are benign. However, some may require further evaluation with ultrasound, and FNAC to determine if they are cancerous. It is important not to ignore a growing or suspicious lump in the neck.
Yes, thyroid cancer can recur, even after successful treatment. Recurrence may happen in the neck or elsewhere in the body. This is why long-term follow-up with your endocrinologist is crucial. Additionally, regular blood tests, and imaging help detect any signs of recurrence early.
If you have had a total thyroidectomy, you will need to take thyroid hormone replacement (levothyroxine) for life. This replaces the hormones your thyroid used to produce, and helps keep your body’s metabolism in balance.
Thyroid cancer involves the uncontrolled growth of abnormal cells, whereas most thyroid conditions, like hypothyroidism, hyperthyroidism or goitres, are non-cancerous, and due to hormonal imbalances or inflammation. Meanwhile, cancer requires specialised treatment, often including surgery, and radioactive iodine therapy.
Most thyroid cancers are not inherited, but some rare types, especially medullary thyroid carcinoma (MTC), may run in families. If you have a family history of thyroid cancer or MEN2 syndromes, genetic counselling, and testing may be recommended.
Thyroid cancer generally has a high survival rate, especially for papillary, and follicular types. According to global data, the 5-year survival rate exceeds 98% for early-stage papillary thyroid cancer. However, outcomes depend on the cancer type, stage, and the individual’s overall health.
While no specific diet can cure thyroid cancer, maintaining a healthy lifestyle, including balanced nutrition, regular exercise, and stress management, can support recovery, and overall well-being.
chat with us
Welcome to The Metabolic Clinic
Holistic Care for Hormones, Bones, and Metabolic Health
Dr Dinesh graduated with honours from Monash University, Melbourne in 2009, receiving the Prince Henry's Prize in Surgery. During his endocrinology training in Melbourne, he won the top registrar award at the Endocrine Society of Australia Clinical Weekend in 2016, followed by securing Australia's only Andrology fellowship in 2017. Upon returning to Singapore, he was the sub-speciality lead for adrenal, pituitary, and bone services at Khoo Teck Puat Hospital and established The Metabolic Bone Clinic.
A passionate educator, he served as Associate Programme Director for Endocrinology at NHG, training the next generation of endocrinologists, and received the NHG Teaching Award for Senior Doctors in 2023. An expert endocrinologist with proficiency in both general and sub-speciality endocrinology, he has an interest in longevity through improving cardiovascular risk, metabolism, bone health, and muscle loss prevention, with the ultimate aim of improving the number of healthy years in one's life.
10+ Years of Experience in Hormone & Metabolic Health
Founder of The Metabolic Bone Clinic in Khoo Teck Puat Hospital
Sub-specialist training with international experts in Melbourne, Australia
Clinical Interest in Longevity & Metabolic Health
START YOUR PERSONALISED HEALTH JOURNEY
If you’re not achieving your treatment targets, struggling with weight changes, fatigue, or unexplained symptoms—it’s time to take a deeper look.
Get clarity with a tailored plan built around you and improving your metabolic health.