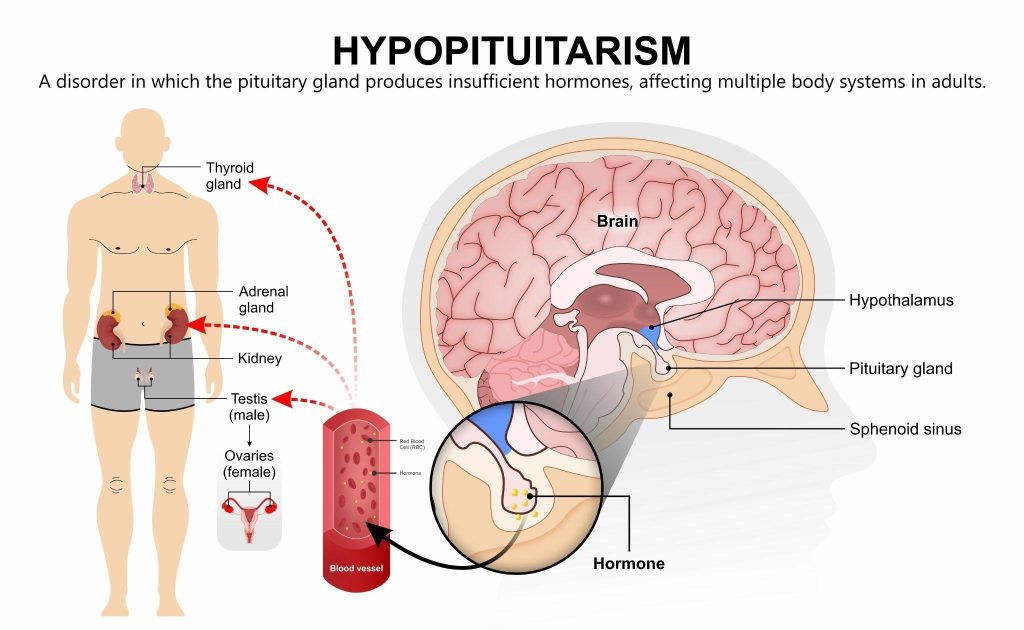
A condition where the pituitary gland does not produce enough hormones, affecting functions such as energy levels, metabolism, growth and reproductive health.
Hypopituitarism is a rare disorder in which the pituitary gland at the base of the brain produces insufficient hormones, disrupting growth, reproduction, metabolism and adrenal function.
What is hypopituitarism?
Hypopituitarism is a rare disorder in which the pituitary gland, a pea-sized structure located at the base of the brain, fails to produce one or more of its essential hormones. Since the pituitary gland controls several other endocrine glands, reduced hormone output can disrupt critical functions such as growth, reproduction, thyroid activity and adrenal response. The severity of symptoms depends on which hormones are affected and whether the deficiency is partial or complete.
Types of hypopituitarism
The condition may involve a single hormone deficiency or multiple hormone deficiencies:
Isolated hormone deficiency — only one hormone is affected. Examples include:
Isolated gonadotropin deficiency — causing menstrual irregularities or infertility in women, and reduced testosterone and fertility problems in men.
Multiple hormone deficiencies (panhypopituitarism) — several or all pituitary hormones are affected. This may result in a combination of adrenal insufficiency, hypothyroidism, infertility, impaired growth and low energy levels.
Congenital hypopituitarism — present from birth, usually due to developmental abnormalities or genetic mutations affecting pituitary function.
Acquired hypopituitarism — more common, developing later in life as a result of pituitary tumours, surgery, radiotherapy, head injury, stroke or inflammatory and autoimmune diseases.
Recognising the type of hypopituitarism is important, as it determines both the symptoms a patient experiences and the treatment required.
What causes hypopituitarism?
Hypopituitarism occurs when the pituitary gland is damaged or its function is disrupted, reducing its ability to release hormones that regulate key body systems. Causes can be present from birth (congenital) or acquired later in life.
Common causes include:
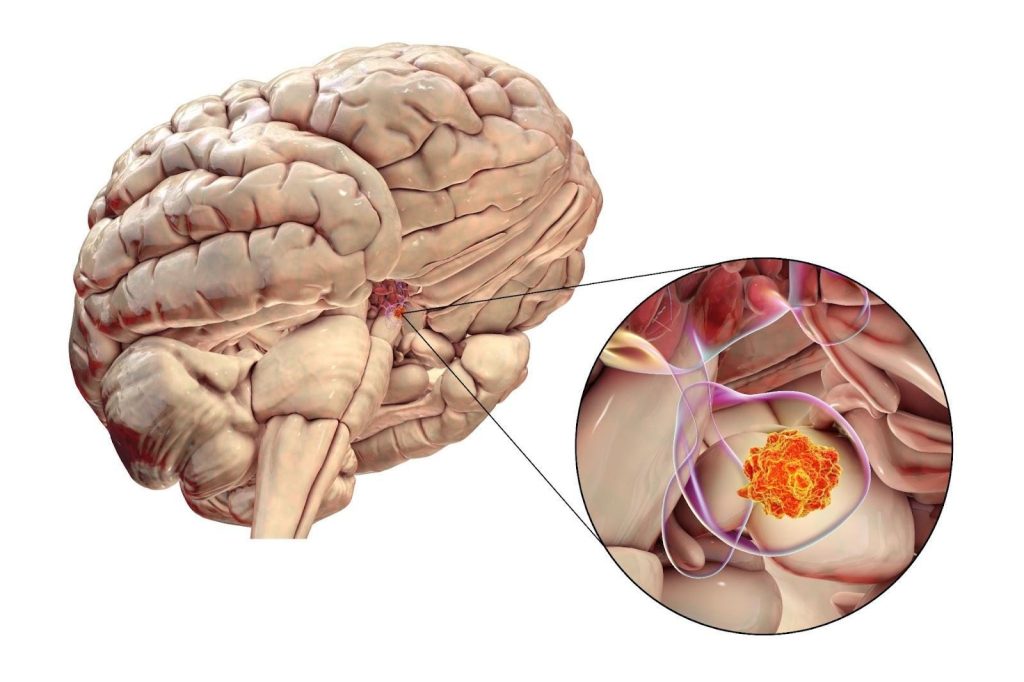
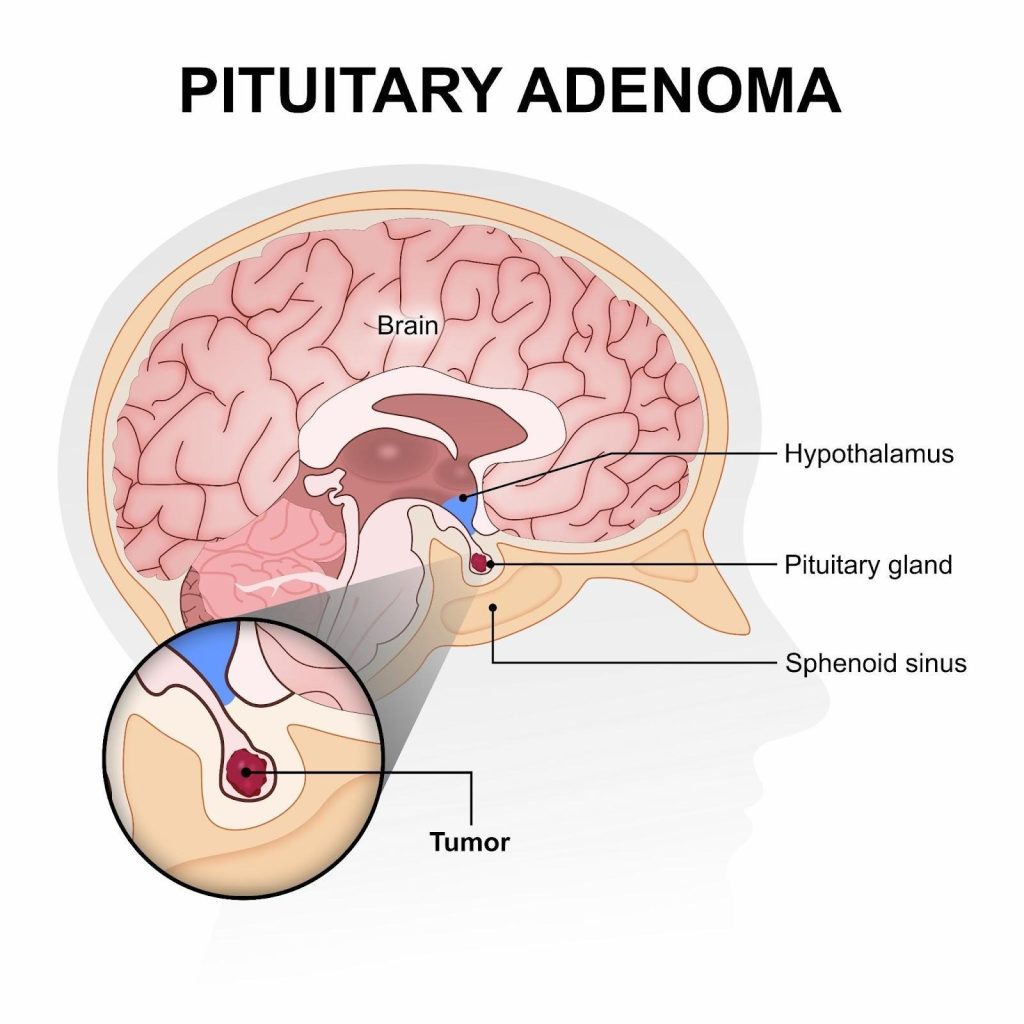
Pituitary tumours — non-cancerous growths (adenomas) are the most frequent cause. They can compress normal pituitary tissue, disrupt hormone production or damage the gland during treatment.
Infections and inflammation — conditions such as meningitis, tuberculosis, sarcoidosis or autoimmune hypophysitis can injure the gland.
Genetic or developmental abnormalities — rare mutations and structural brain differences may cause congenital hypopituitarism.
Other brain conditions — tumours or cysts near the hypothalamus or pituitary stalk can interfere with hormonal signalling.
In many cases, hypopituitarism develops gradually, but in others, such as pituitary apoplexy, it can present suddenly and require urgent medical attention. Identifying the underlying cause is essential to determine the most effective treatment plan.
Pituitary adenoma, a benign tumour in the pituitary gland at the base of the brain, is the most common primary cause of hypopituitarism.
What are the symptoms of hypopituitarism?
The symptoms of hypopituitarism vary widely depending on which pituitary hormones are deficient, how severe the deficiency is and whether the onset is sudden or gradual. Because the pituitary regulates multiple glands, symptoms may affect several body systems at once.
General features — fatigue, weakness, low energy levels, unexplained weight changes, sensitivity to cold and reduced ability to cope with stress are common in many patients.
Hormone-specific symptoms
Adrenocorticotropic hormone (ACTH) deficiency — causes secondary adrenal insufficiency, with fatigue, low blood pressure, dizziness, nausea, abdominal pain and increased risk of adrenal crisis in severe cases.
Thyroid-stimulating hormone (TSH) deficiency — leads to secondary hypothyroidism, with tiredness, cold intolerance, dry skin, constipation and weight gain.
Luteinising hormone (LH) and follicle-stimulating hormone (FSH) deficiency — in women, it may cause irregular or absent periods, infertility, vaginal dryness and reduced libido. In men, it can result in low testosterone, erectile dysfunction, infertility and decreased body hair.
Growth hormone (GH) deficiency — in children, it causes growth failure and delayed puberty. In adults, it leads to reduced muscle mass, increased body fat, decreased bone density and low quality of life.
Prolactin deficiency — rare, but it can impair milk production in women after childbirth.
Antidiuretic hormone (ADH) deficiency (if hypothalamic involvement is present) — may cause diabetes insipidus, with excessive thirst and frequent urination.
Because symptoms often develop slowly, hypopituitarism can go unrecognised for years. A high level of suspicion and proper testing are essential for diagnosis.
What are the complications of hypopituitarism?
Hypopituitarism can affect multiple body systems at once, as the pituitary gland regulates hormones involved in growth, metabolism, stress response, and reproductive function.
If left untreated, hypopituitarism can lead to serious health consequences because of the wide-ranging effects of pituitary hormone deficiencies. Complications depend on the hormones involved and the duration of untreated disease.
Adrenal insufficiency — lack of ACTH leads to reduced cortisol production, which can cause life-threatening adrenal crises during illness, injury or surgery if not managed promptly.
Hypothyroidism — TSH deficiency results in low thyroid hormone levels, increasing the risk of cardiovascular disease, high cholesterol, weight gain and reduced quality of life.
Reproductive and fertility issues — Deficiency of LH and FSH may cause infertility, menstrual disturbances in women, erectile dysfunction in men and complications during pregnancy if untreated.
Skeletal and metabolic effects — growth hormone deficiency in adults contributes to osteoporosis, reduced muscle strength, increased body fat and higher risk of cardiovascular disease. In children, untreated GH deficiency leads to stunted growth and delayed development.
Vision and neurological problems — when hypopituitarism is caused by a large pituitary tumour, pressure on nearby structures can cause headaches, visual field loss or other neurological symptoms.
Reduced quality of life and increased mortality — long-term untreated hypopituitarism is linked with higher rates of disability, impaired daily functioning and increased mortality, especially when adrenal or thyroid hormone deficiencies are present.
With proper diagnosis, hormone replacement therapy and regular monitoring, most of these complications can be prevented or effectively managed.
Who is at risk of hypopituitarism in Singapore?
Hypopituitarism is uncommon, but certain groups of people are more likely to develop the condition because of underlying medical issues or treatments affecting the pituitary gland.
People with pituitary or brain tumours — non-cancerous pituitary adenomas are the leading cause. Larger tumours can compress normal pituitary tissue, while treatment for tumours (surgery or radiotherapy) can also damage the gland.
Individuals with a history of head injury or brain surgery — traumatic brain injury, cranial surgery, or procedures near the hypothalamus and pituitary region can disrupt hormone production.
Patients exposed to radiotherapy — radiotherapy for brain tumours, nasal cancers or pituitary disease increases the risk of delayed pituitary hormone deficiency, sometimes years after treatment.
Those with vascular events — people who have had pituitary apoplexy (sudden bleeding into a pituitary tumour) or Sheehan’s syndrome (pituitary damage following severe blood loss during childbirth) are at higher risk.
Individuals with chronic medical or inflammatory conditions — autoimmune hypophysitis, infections such as meningitis or tuberculosis and systemic diseases like sarcoidosis can damage the pituitary.
People with genetic or congenital factors — though rare, some are born with pituitary developmental abnormalities or genetic mutations that impair pituitary function from birth.
How is hypopituitarism diagnosed?
Diagnosing hypopituitarism requires a thorough evaluation of medical history, physical symptoms, hormone testing and imaging studies. Because the condition can develop gradually and mimic other illnesses, careful assessment is essential.
Medical history and examination — doctors will review symptoms such as fatigue, menstrual irregularities, infertility, low libido or growth failure in children. A physical examination may reveal signs of hormone deficiency, such as low blood pressure, reduced body hair or delayed puberty.
Hormone testing — blood tests are central to diagnosis. These measure levels of pituitary hormones (such as ACTH, TSH, LH, FSH, GH, and prolactin) along with the hormones they regulate (thyroid hormones, cortisol, oestrogen, testosterone and insulin-like growth factor-1). Special stimulation or suppression tests may be performed to check how the pituitary responds under controlled conditions.
Imaging studies — MRI scans of the brain and pituitary gland help detect tumours, structural abnormalities or damage that could explain the hormone deficiencies.
Other investigations — In selected cases, genetic testing or further blood work may be recommended, especially when congenital hypopituitarism is suspected.
Combining hormone analysis with imaging ensures an accurate diagnosis and helps identify whether the condition is due to a tumour, injury, congenital cause or other disease.
What are the treatment options for hypopituitarism in Singapore?
Treatment focuses on replacing the missing hormones, managing the underlying cause where possible and preventing long-term complications. Because hypopituitarism often affects several hormones, lifelong therapy and monitoring are usually required.
Hormone replacement therapy
Cortisol replacement — hydrocortisone is prescribed to replace cortisol when ACTH deficiency is present. Doses may need to be increased during illness, surgery, or stress to prevent adrenal crisis.
Sex hormone replacement— oestrogen and progesterone in women (unless contraindicated) and testosterone in men restore sexual function, bone strength, and general well-being.
Growth hormone (GH) therapy — recombinant GH may be prescribed for children with growth failure or adults with reduced muscle mass, bone density, and quality of life.
Fertility treatment — specialised hormone injections can stimulate ovulation in women or sperm production in men if fertility is desired.
Treatment of underlying causes
Pituitary tumours may require surgery, radiotherapy or medication.
Inflammatory or autoimmune conditions may be managed with immunosuppressive therapy.
Vascular events, such as pituitary apoplexy, require urgent treatment and long-term hormone replacement.
Monitoring and follow-up
Regular blood tests, imaging when needed and adjustments in hormone doses are essential to ensure stability. Patients are also advised to carry medical alert identification for emergencies, particularly if they require cortisol replacement.
With appropriate treatment and lifelong care, most people with hypopituitarism can live healthy, active lives.
Prognosis and long-term outlook for hypopituitarism
With timely diagnosis and appropriate hormone replacement, many people with hypopituitarism can lead healthy and fulfilling lives. The long-term outlook depends on the underlying cause, the number of hormones affected and how well treatment is maintained.
Lifelong management — most patients require ongoing hormone replacement and regular follow-up. Adjustments in medication are often necessary, especially during times of illness, surgery or major life changes.
Quality of life — when treatment is well balanced, symptoms such as fatigue, low libido and mood changes can improve significantly. Growth hormone therapy may further enhance bone strength, muscle mass and energy in selected patients.
Risks and complications — if untreated, hypopituitarism can lead to life-threatening adrenal crises, severe hypothyroidism, infertility, osteoporosis and reduced life expectancy. Even with treatment, some individuals may have a slightly higher risk of cardiovascular disease and metabolic problems, which highlights the need for close monitoring.
Overall outlook — advances in hormone replacement therapy and imaging have improved outcomes considerably. With expert care, most patients achieve stable health, maintain independence and enjoy a good quality of life.
Summary
Hypopituitarism is a rare but serious disorder in which the pituitary gland fails to produce one or more essential hormones, leading to wide-ranging effects on growth, reproduction, thyroid function, adrenal response and overall well-being. It may develop gradually or suddenly, most often due to tumours, surgery, head injury or other medical conditions. With accurate diagnosis, appropriate hormone replacement and ongoing monitoring, hypopituitarism can be managed effectively, allowing patients to maintain good health and quality of life.
If you are experiencing symptoms such as persistent fatigue, unexplained weight changes, low libido or changes in menstrual or sexual function, schedule a consultation with The Metabolic Clinic for comprehensive assessment, tailored treatment and long-term support.
No. Hypopituitarism refers to hormone deficiency due to pituitary underactivity, while pituitary tumours are one of several possible causes of hypopituitarism, they aren’t the same.
Yes. Although it often develops gradually, hypopituitarism can occur suddenly after pituitary apoplexy, head trauma or severe blood loss during childbirth (Sheehan’s syndrome).
Yes. In children, hypopituitarism may cause growth failure, delayed puberty or developmental issues, while in adults it typically causes fatigue, low libido and metabolic problems.
If untreated, severe hormone deficiencies, especially of cortisol (secondary adrenal insufficiency), can be life-threatening. With treatment, the risks are greatly reduced.
No. Some people have isolated deficiencies (e.g., only growth hormone or gonadotropins), while others have multiple hormone deficiencies (panhypopituitarism).
No. Hypopituitarism is considered a rare condition, though it may be underdiagnosed because symptoms develop gradually and overlap with other illnesses.
Yes. Sheehan’s syndrome, a rare complication of severe postpartum bleeding, can cause hypopituitarism in women after childbirth due to injury of the pituitary gland.
If untreated, yes, due to complications such as adrenal crisis or cardiovascular disease. With proper hormone replacement, most patients live normal lives.
Dr Dinesh graduated with honours from Monash University, Melbourne in 2009, receiving the Prince Henry's Prize in Surgery. During his endocrinology training in Melbourne, he won the top registrar award at the Endocrine Society of Australia Clinical Weekend in 2016, followed by securing Australia's only Andrology fellowship in 2017. Upon returning to Singapore, he was the sub-speciality lead for adrenal, pituitary, and bone services at Khoo Teck Puat Hospital and established The Metabolic Bone Clinic.
A passionate educator, he served as Associate Programme Director for Endocrinology at NHG, training the next generation of endocrinologists, and received the NHG Teaching Award for Senior Doctors in 2023. An expert endocrinologist with proficiency in both general and sub-speciality endocrinology, he has an interest in longevity through improving cardiovascular risk, metabolism, bone health, and muscle loss prevention, with the ultimate aim of improving the number of healthy years in one's life.
10+ Years of Experience in Hormone & Metabolic Health
Founder of The Metabolic Bone Clinic in Khoo Teck Puat Hospital
Sub-specialist training with international experts in Melbourne, Australia
Clinical Interest in Longevity & Metabolic Health
START YOUR PERSONALISED HEALTH JOURNEY
If you’re not achieving your treatment targets, struggling with weight changes, fatigue, or unexplained symptoms—it’s time to take a deeper look.
Get clarity with a tailored plan built around you and improving your metabolic health.