A prolactinoma is a benign (non-cancerous) tumour of the pituitary gland that produces excessive amounts of prolactin, a hormone responsible for regulating reproductive function, fertility and milk production after childbirth.
Prolactinoma is a benign pituitary tumour that causes excessive prolactin production, leading to hormonal imbalance and reproductive issues in both men and women.
What is a prolactinoma?
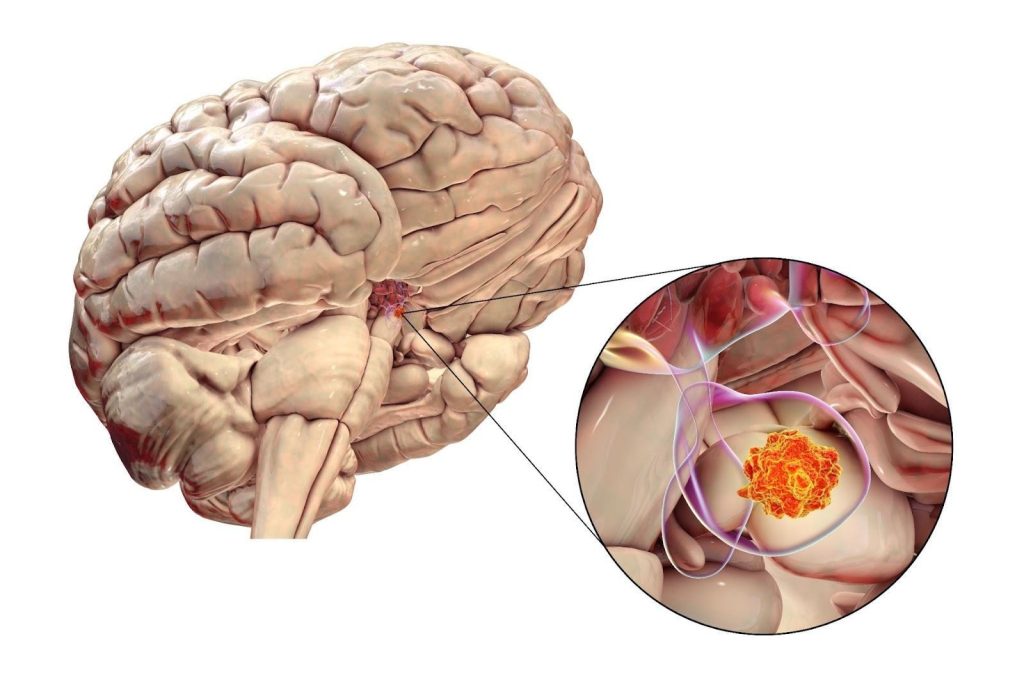
A prolactinoma is a benign (non-cancerous) tumour of the pituitary gland that produces excessive amounts of prolactin, a hormone responsible for regulating reproductive function, fertility and milk production after childbirth. The pituitary gland, located at the base of the brain, controls several key hormones, and when a tumour develops, it can interfere with normal hormonal balance and nearby structures.
Excess prolactin disrupts the normal production of sex hormones: oestrogen in women and testosterone in men, leading to symptoms such as menstrual irregularities, infertility, reduced libido and, in more severe cases, abnormal breast milk production (galactorrhoea).
Types of prolactinomas
Prolactinomas are classified by size and the extent to which they affect surrounding tissues:
Microprolactinoma — a small tumour less than 10 millimetres in diameter. These are more common in women and often detected early due to menstrual changes or infertility.
Macroprolactinoma — a larger tumour greater than 10 millimetres. These are more common in men and may cause additional symptoms such as headaches and vision problems due to pressure on nearby structures like the optic nerves.They are more common in men because they become symptomatic later than in women where menstrual irregularities allow this to be picked up earlier.
Giant prolactinoma — an exceptionally large prolactin-secreting tumour typically measuring more than 40 millimetres. These can extend beyond the pituitary region into surrounding areas and are more likely to cause significant pressure-related symptoms such as persistent headaches, visual disturbance or hormonal imbalances due to compression of nearby structures.
Most prolactinomas grow slowly and remain confined to the pituitary gland. Although they are not malignant, their hormonal effects and local pressure can cause significant symptoms if untreated. Early diagnosis and appropriate management are important to restore hormonal balance, protect vision and preserve fertility. As the only pituitary tumor that can be treated wthout surgery, it is important to diagnose.
What causes prolactinomas?
The exact cause of prolactinomas is not fully understood. In most cases, it develops spontaneously when cells in the pituitary gland that produce prolactin (lactotroph cells) multiply more than normal, forming a benign tumour. Although these tumours are non-cancerous and rarely spread, they can interfere with normal pituitary function and disrupt hormonal balance through excess prolactin secretion.
Genetic factors
A small proportion of prolactinomas occur as part of inherited conditions, particularlymultiple endocrine neoplasia type 1 (MEN 1). This rare syndrome predisposes individuals to develop tumours in several endocrine glands, including the pituitary, parathyroid and pancreas.
Other causes of a high prolactin level (Hyperprolactinaemia)
In rare cases, prolactin levels may also rise due to:
Medications — certain drugs used for schizophrenia, depression, high blood pressure, or nausea can increase prolactin release.
Hypothalamic disorders — conditions affecting the brain region that regulates prolactin can mimic the effects of a prolactinoma.
Non-functional pituitary adenoma- these tumors do not produce prolactin, but interfere with the regulation of prolactin release and call mild prolactin elevations.
While many factors can cause elevated prolactin (a condition called hyperprolactinaemia), a prolactinoma refers specifically to a prolactin-secreting tumour within the pituitary gland. Distinguishing between these causes is crucial for accurate diagnosis and treatment planning.
What are the symptoms of prolactinoma?
The symptoms of prolactinoma arise mainly from two factors:
excessive prolactin production, which disrupts reproductive hormones and
the size or pressure effects of the tumour itself.
Symptoms can differ between women and men because of the hormone changes involved and the typical size at diagnosis.
Prolactinoma symptoms in women
Symptoms often appear early when the tumour is still small (microprolactinoma) because of changes in menstrual and reproductive function. Common features include:
Irregular or absent menstrual periods (amenorrhoea)
Difficulty becoming pregnant due to ovulation problems
Reduced libido or vaginal dryness
Milk discharge from the breasts (galactorrhoea) unrelated to childbirth or breastfeeding
Prolactinoma symptoms in men
Prolactinomas are usually diagnosed later and tend to be larger (macroprolactinomas). Symptoms may include:
Reduced libido and erectile dysfunction
Infertility or low sperm count
Loss of body or facial hair
Breast enlargement (gynaecomastia)
Symptoms from tumour pressure
When a macroprolactinoma presses on nearby structures, additional symptoms can occur in both sexes:
Persistent headaches
Visual disturbances, particularly loss of peripheral vision
Rarely, double vision or other neurological symptoms
Because these signs can develop gradually, prolactinomas may remain undiagnosed for years. Recognising early hormonal symptoms is key to timely evaluation and effective treatment.
Who is at risk of prolactinoma in Singapore?
Prolactinomas can occur in both men and women, but certain groups are more likely to develop the condition. Recognising who is at risk helps guide early testing and intervention before complications arise.
Sex and age — prolactinomas are more common in women between the ages of 20 and 50, typically appearing during the reproductive years. In men, the condition is less common but tumours tend to be larger (macroprolactinomas) at the time of diagnosis because symptoms often appear later and thus it is harder to pick-up tumours when they are smaller in men.
Family history — individuals with a family history of multiple endocrine neoplasia type 1 (MEN1) are at higher risk. This genetic condition increases the likelihood of developing pituitary, pancreatic and parathyroid tumours.
Endocrine disorders — people with untreated hypothyroidism or other pituitary abnormalities are at greater risk of developing elevated prolactin levels or secondary pituitary changes.
Certain medications — long-term use of drugs that affect dopamine, such as some antipsychotics, antidepressants or blood pressure medicines, can increase prolactin levels and may contribute to tumour development in rare cases.
Although most prolactinomas occur without an identifiable cause, individuals with the above risk factors benefit from comprehensive hormonal evaluation and early medical assessment if symptoms develop.
How is a prolactinoma diagnosed?
Diagnosis of a prolactinoma involves confirming excess prolactin levels, ruling out other possible causes of hyperprolactinaemia and identifying the presence of a pituitary tumour. A combination of blood tests, imaging and clinical evaluation is used to ensure accuracy.
Blood tests — measurement of serum prolactin levels is the first step. Persistently high prolactin levels suggest overproduction by the pituitary gland. A phenomenon called macroprolactin needs to be ruled out (a false cause of high prolactin that is benign). Additional hormone tests, such as thyroid, cortisol and sex hormone levels help exclude other conditions that can raise prolactin or result from pituitary dysfunction.
Imaging studies — a magnetic resonance imaging (MRI) scan of the brain is used to visualise the pituitary gland and detect the presence, size and extent of a tumour. MRI can distinguish between microprolactinomas (small) and macroprolactinomas (large) and assess whether nearby structures, such as the optic nerves, are affected.
Visual field testing — when a large tumour is suspected, an eye examination is performed to check for loss of peripheral vision caused by compression of the optic chiasm.
Additional investigations — in selected cases, genetic testing may be offered if an inherited condition such as MEN1 is suspected.
A clear diagnosis ensures that treatment can be tailored precisely to the tumour’s size, the degree of hormonal disturbance and the patient’s reproductive and general health needs.
What are the treatment options for prolactinomas in Singapore?
The main goal of treatment is to reduce prolactin levels, restore normal hormone balance, shrink the tumour and relieve any pressure on nearby structures such as the optic nerves. Most prolactinomas respond very well to medical therapy, with surgery or radiotherapy reserved for specific situations.
Medical treatment
Dopamine agonists are the most commonly used therapy for prolactinomas. These medications (such as cabergoline or bromocriptine) act by stimulating dopamine receptors, which naturally suppress prolactin production. In most patients, they normalise prolactin levels, restore fertility and reduce or even eliminate the tumour.
Regular monitoring through blood tests and MRI scans helps assess response and guide dosage adjustments.
Many patients remain on long-term therapy, although some with stable prolactin levels may eventually be able to taper their dose under medical supervision.
Surgical treatment
Surgery may be considered when medical therapy is ineffective, poorly tolerated or when the tumour causes pressure on the optic nerves and threatens vision.
The procedure, known as transsphenoidal surgery, removes the tumour through the nasal passage without external incisions. It is generally safe and effective when performed by an experienced neurosurgeon.
Radiotherapy
Radiation treatment is rarely required and is reserved for cases where both medication and surgery fail to control the tumour.
Modern stereotactic techniques can target the tumour precisely while minimising damage to surrounding brain tissue.
Ongoing management
Long-term follow-up is essential, as prolactinomas can recur even after successful treatment. Periodic hormone testing and MRI imaging ensure that prolactin levels remain stable and the tumour does not regrow.
With timely diagnosis and appropriate therapy, most patients achieve excellent outcomes, regaining hormonal balance and quality of life.
Prognosis and long-term outlook for prolactinoma
With early diagnosis and effective treatment, the long-term outlook for prolactinoma is generally excellent. Most patients respond well to medication, achieving normal prolactin levels, tumour shrinkage and restoration of reproductive and hormonal function.
Response to treatment — dopamine agonists successfully control prolactin levels in the majority of patients, often within weeks of starting therapy. Tumour size usually decreases significantly and symptoms such as menstrual irregularities, galactorrhoea and sexual dysfunction typically improve or resolve.
Fertility and hormonal recovery — in women, fertility often returns once prolactin levels normalise and in men, testosterone levels and libido usually improve. Patients planning pregnancy are closely monitored, as microprolactinomas can enlarge slightly during gestation.
Surgical and long-term outcomes — for those requiring surgery, outcomes are generally favourable, particularly for smaller tumours. However, long-term follow-up is crucial, as prolactin levels may rise again over time. Some patients require lifelong medication to keep the tumour controlled.
Quality of life and monitoring — most individuals lead normal lives with minimal restrictions once treatment is established. Regular endocrinology reviews, blood tests and occasional MRI scans are recommended to ensure continued hormonal stability and early detection of recurrence.
Overall, prolactinoma is a highly treatable condition. With consistent medical care and monitoring, long-term control is achievable and complications are uncommon.
Summary
Prolactinoma is a benign pituitary tumour that causes excessive prolactin secretion, disrupting reproductive hormones and, in some cases, pressing on nearby structures such as the optic nerves. Although its symptoms can be wide-ranging, from menstrual irregularities and infertility to headaches and visual changes, it is one of the most treatable pituitary disorders.
Accurate diagnosis through hormone testing and MRI scanning allows for early, targeted management. Most patients respond extremely well to dopamine-agonist medication, which can normalise prolactin levels, restore fertility and shrink the tumour. Surgery and radiotherapy are effective options when medical therapy alone is insufficient. With ongoing monitoring and specialist care, long-term control and an excellent quality of life are achievable.
If you have symptoms suggestive of a pituitary disorder or have been diagnosed with high prolactin levels, schedule a consultation with The Metabolic Clinic for professional evaluation, a detailed diagnosis and comprehensive management tailored to improve your condition.
No. A prolactinoma is a benign (non-cancerous) tumour of the pituitary gland. It does not spread to other parts of the body but can cause symptoms through excess hormone production or local pressure.
The exact cause of prolactinoma is unknown, but it results from overgrowth of prolactin-producing cells in the pituitary gland called lactotrophs. Rarely, it may be linked to genetic conditions such as multiple endocrine neoplasia type 1 (MEN1).
Prolactinoma is the most common type of pituitary tumour. It occurs more frequently in women of reproductive age but can also affect men and older adults.
Yes. High prolactin levels suppress reproductive hormones, leading to irregular menstrual cycles in women and reduced testosterone levels and sperm production in men, both of which can cause infertility.
Yes. Women often develop smaller tumours (microprolactinomas) that present earlier with menstrual changes, while men typically are diagnosed with larger tumours (macroprolactinomas) as they have symptoms later in the disease course.
Most cases can be controlled very effectively with medication. In many patients, prolactin levels return to normal and the tumour shrinks, though long-term follow-up is required.
Dopamine agonists such as cabergoline or bromocriptine are commonly prescribed to lower prolactin levels, restore fertility and reduce tumour size in patients with prolactinoma.
Surgery is considered if the tumour does not respond to medication, if vision is threatened or if a patient cannot tolerate medical therapy. The operation is usually performed through the nasal passage (transsphenoidal surgery).
Most women with microprolactinomas can have a safe pregnancy under medical supervision. Prolactin levels naturally rise during pregnancy, so close monitoring is important.
Some patients experience fatigue, low energy or mild weight gain due to hormonal imbalance, particularly when testosterone or oestrogen levels are low.
Dr Dinesh graduated with honours from Monash University, Melbourne in 2009, receiving the Prince Henry's Prize in Surgery. During his endocrinology training in Melbourne, he won the top registrar award at the Endocrine Society of Australia Clinical Weekend in 2016, followed by securing Australia's only Andrology fellowship in 2017. Upon returning to Singapore, he was the sub-speciality lead for adrenal, pituitary, and bone services at Khoo Teck Puat Hospital and established The Metabolic Bone Clinic.
A passionate educator, he served as Associate Programme Director for Endocrinology at NHG, training the next generation of endocrinologists, and received the NHG Teaching Award for Senior Doctors in 2023. An expert endocrinologist with proficiency in both general and sub-speciality endocrinology, he has an interest in longevity through improving cardiovascular risk, metabolism, bone health, and muscle loss prevention, with the ultimate aim of improving the number of healthy years in one's life.
10+ Years of Experience in Hormone & Metabolic Health
Founder of The Metabolic Bone Clinic in Khoo Teck Puat Hospital
Sub-specialist training with international experts in Melbourne, Australia
Clinical Interest in Longevity & Metabolic Health
START YOUR PERSONALISED HEALTH JOURNEY
If you’re not achieving your treatment targets, struggling with weight changes, fatigue, or unexplained symptoms—it’s time to take a deeper look.
Get clarity with a tailored plan built around you and improving your metabolic health.