A hormonal imbalance that affects ovulation, menstrual regularity and androgen levels, often linked to acne, weight changes and fertility concerns.
What is polycystic ovary syndrome (PCOS)?
Polycystic Ovary Syndrome (PCOS) is a chronic hormonal disorder that affects how the ovaries function. It is one of the most common endocrine conditions among individuals of reproductive age, affecting an estimated 1 in 10 women globally. Despite the name, not everyone with PCOS has ovarian cysts.
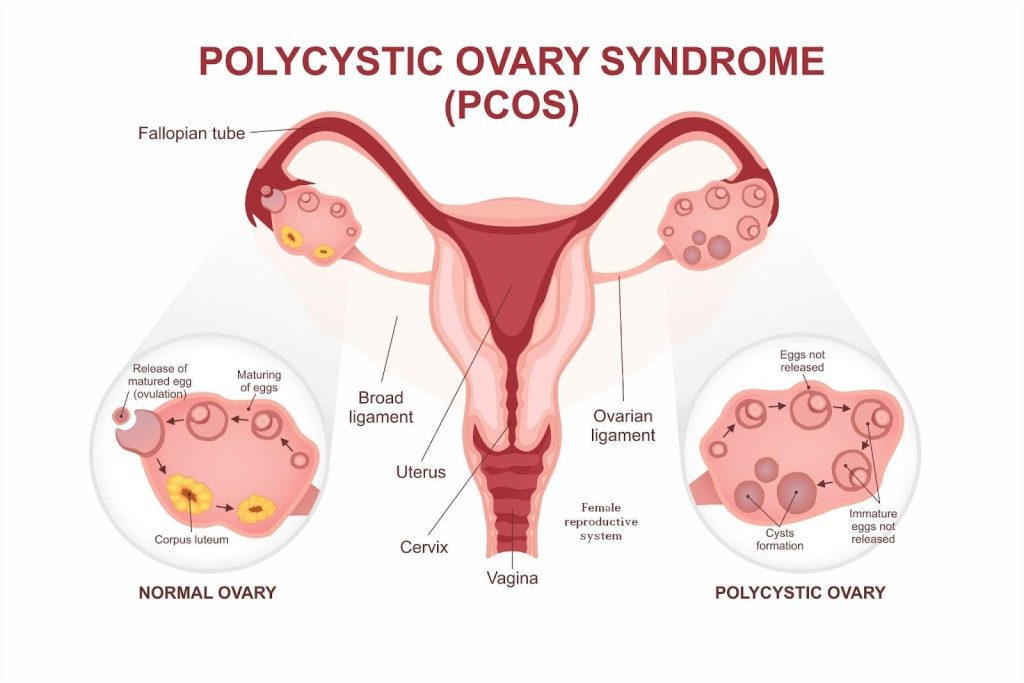
The condition is typically defined by a combination of three key features: irregular or absent ovulation, excess androgen (male hormone) levels, and polycystic ovaries visible on ultrasound. According to the widely accepted Rotterdam criteria, a diagnosis is made when two out of these three features are present, after ruling out other possible causes. Recently a high AMH (Anti-mullerian hormone) level has been added into the diagnostic criteria as a surrogate blood test marker of polycystic ovaries.
In PCOS, hormonal imbalances disrupt the normal menstrual cycle and ovulation process. The ovaries may produce excess androgens such as testosterone, which can lead to physical symptoms like acne, excessive facial or body hair (hirsutism), and male-pattern hair thinning. Additionally, many individuals with PCOS have insulin resistance which is postulated as one of the causes of PCOS and increases the risk of type 2 diabetes over time.
While PCOS is primarily known for its impact on menstrual health and fertility, it also has broader metabolic and psychological implications particularly due to skin changes (Acne). It is associated with a higher risk of conditions such as insulin resistance, dyslipidemia, endometrial hyperplasia, and mood disorders like anxiety and depression. Early diagnosis and management are essential for reducing long-term health risks and improving quality of life.
In PCOS, the ovaries fail to release mature eggs regularly, leading to the buildup of multiple immature follicles and the formation of cyst-like structures.
What causes polycystic ovary syndrome (PCOS)?
The exact cause of PCOS is not fully understood, but it is believed to result from a combination of hormonal imbalances and inherited traits that disrupt ovarian function. Several interconnected mechanisms contribute to the development and progression of the condition:
Insulin resistance — a significant number of individuals with PCOS have insulin resistance, where the body’s cells don’t respond properly to insulin. This prompts the pancreas to produce more insulin, which can stimulate the ovaries to secrete excess androgens (male hormones), leading to irregular ovulation and visible symptoms such as acne or hirsutism. It may also have central effects on the reproductive hormonal axis as well.
Excess androgen production — women with PCOS often produce elevated levels of androgens, either from the ovaries or adrenal glands. These hormones interfere with the normal development of ovarian follicles, preventing ovulation and contributing to symptoms like hair thinning or oily skin.
Chronic low-grade inflammation — many individuals with PCOS show signs of persistent, low-level inflammation in the body. This inflammation may contribute to increased androgen production and is also associated with a higher risk of cardiovascular issues and insulin resistance.
Genetic predisposition — PCOS often runs in families, indicating a heritable component. If a close female relative has PCOS, the likelihood of developing the condition increases, although the exact genes involved have not yet been clearly identified.
Prenatal hormonal exposure — some studies suggest that exposure to high androgen levels in the womb may influence fetal development in ways that increase the risk of PCOS later in life, though this area remains under investigation.
Lifestyle factors like weight gain or lack of physical activity do not cause PCOS on their own but can worsen insulin resistance and hormonal imbalances, intensifying symptoms and long-term health risks.
What are the symptoms of polycystic ovary syndrome (PCOS)?
PCOS presents differently in each individual, but most symptoms stem from hormonal imbalances, particularly elevated androgens and disrupted ovulation. The symptoms may begin around puberty or develop later, especially after significant weight gain. Common signs include:
Irregular or missed periods — due to disrupted ovulation, individuals with PCOS often have infrequent, unpredictable, or prolonged menstrual cycles. Some may experience fewer than 9 periods per year or have cycles longer than 35 days.
Excess hair growth (hirsutism) — elevated androgen levels can cause coarse, dark hair to grow on the face, chest, abdomen, or back, affecting up to 70–80% of women with PCOS.
Acne and oily skin — increased androgens can overstimulate oil glands, leading to persistent or severe acne, particularly on the face, chest, and upper back.
Hair thinning or male-pattern hair loss — some individuals may notice thinning hair at the crown or along the hairline, similar to androgenic alopecia.
Weight gain or difficulty losing weight — many people with PCOS experience weight gain, particularly around the abdomen, due to underlying insulin resistance.
Polycystic ovaries — on ultrasound, the ovaries may appear enlarged and contain multiple small follicles (often mislabelled as “cysts”) that fail to mature and release eggs regularly.
Skin changes — darkened, velvety patches of skin (acanthosis nigricans) may develop in body folds like the neck, armpits, or groin, often associated with insulin resistance.
Mood and mental health symptoms — depression, anxiety, low self-esteem, and body image concerns are more common among individuals with PCOS.
Not everyone with PCOS experiences all of these symptoms, and their severity can vary widely. Early recognition and appropriate management can help reduce long-term complications and improve overall well-being.
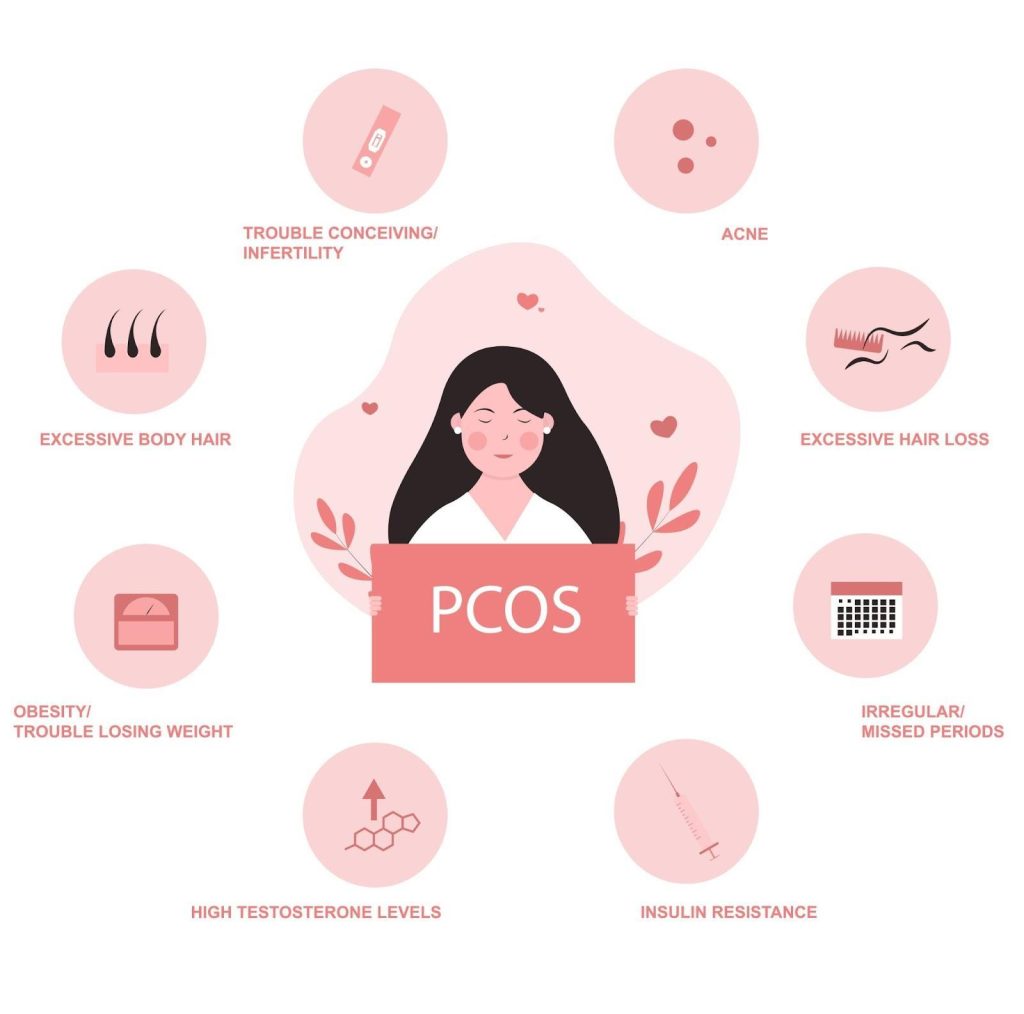
PCOS may cause irregular periods, acne, excessive body or facial hair, scalp hair thinning, weight gain, infertility, and insulin resistance.
What happens if a woman has PCOS?
PCOS is more than a hormonal imbalance; iif left unmanaged, it can lead to serious long-term health complications. The effects may not be immediately visible, but over time, the condition can interfere with a woman’s reproductive, metabolic, and emotional well-being. Some of the key consequences include:
Infertility and ovulation issues — irregular or absent ovulation often makes it difficult to conceive, making PCOS one of the leading causes of infertility.
Increased risk of type 2 diabetes — insulin resistance, common in PCOS, significantly raises the likelihood of developing diabetes at a younger age.
Higher chance of endometrial cancer — prolonged absence of menstruation can lead to thickening of the uterine lining (endometrial hyperplasia), increasing the risk of cancer over time.
Pregnancy complications — women with PCOS are more likely to experience gestational diabetes, preeclampsia, preterm birth, and miscarriage.
Long-term weight challenges — difficulty losing weight and a tendency to gain weight easily can persist, increasing the risk of obesity-related complications.
PCOS requires long-term attention not just to treat the symptoms, but to prevent these broader complications. With the right care plan, many of these risks can be reduced or avoided.
Who is at risk of polycystic ovary syndrome (PCOS) in Singapore?
PCOS affects around 10–13% of women of reproductive age in Singapore. While it can occur in anyone with ovaries, certain risk factors increase the chances of developing this condition. These include:
Family history — women are more likely to develop PCOS if their mother, sister, or close female relative also has it. There is a strong genetic component.
Excess weight and insulin resistance — being overweight or obese, especially with fat concentrated around the abdomen, increases insulin resistance. This in turn stimulates the ovaries to produce more androgens, disrupting ovulation.
Sedentary lifestyle and poor diet — a lack of physical activity and high intake of processed or sugary foods can worsen insulin resistance, especially in urban settings like Singapore where desk-bound routines and fast food are common.
Hormonal or intrauterine factors — some evidence suggests that prenatal exposure to excess androgens or endocrine-disrupting chemicals may increase the likelihood of developing PCOS later in life.
If you have any of the above risk factors, especially alongside irregular periods, acne, or unwanted hair growth, it’s worth speaking to a doctor. Early identification can help reduce the risk of long-term health problems and improve hormonal and metabolic balance.
How is polycystic ovary syndrome (PCOS) diagnosed?
There is no single test for PCOS. Diagnosis is made based on a combination of clinical signs, blood tests, and imaging studies. We follow the 2023 International Evidence-Based Guideline for the assessment and management of PCOS, which require any two of the following three features to confirm a diagnosis, after excluding other causes:
Irregular or absent ovulation — this is typically seen as infrequent periods (fewer than 9 a year), prolonged cycles (more than 35 days), or missed periods.
Excess androgen levels — these may be observed as physical signs (such as acne, hirsutism, or scalp hair thinning) or confirmed through blood tests showing elevated testosterone or DHEAS.
Polycystic ovaries on ultrasound — an internal pelvic ultrasound may show enlarged ovaries with multiple small follicles (more than 20 per ovary) or increased ovarian volume. Serum AMH may be used as a surrogate marker.
Because PCOS can look different in different people and other medical conditions can masquerade as PCOS, a full clinical history and physical examination are essential for accurate diagnosis and personalised management.
Additional tests may be ordered to rule out other conditions that mimic PCOS, such as thyroid disorders, elevated prolactin, or adrenal abnormalities. Blood tests often include fasting glucose, lipid profile, and hormone panels to assess overall reproductive and metabolic health.
What are the treatment options for polycystic ovary syndrome (PCOS) in Singapore?
There is no universal cure for PCOS, but symptoms and risks can be managed effectively with a personalised care plan. Treatment for PCOS depends on your specific concerns, whether it’s irregular periods, acne, fertility, weight issues, or long-term metabolic health. The main treatment options include:
Lifestyle modifications — Major treatment for most individuals with PCOS
Lifestyle changes can significantly improve hormonal balance, insulin sensitivity, menstrual regularity, and fertility.
Weight loss — losing 5–10% of body weight can help restore ovulation, reduce androgen levels, and regulate menstrual cycles.
Balanced diet — a low-glycemic index diet that includes lean proteins, whole grains, fruits, vegetables, and healthy fats supports better blood sugar control.
Regular exercise — at least 150 minutes per week of moderate-intensity exercise (like brisk walking, cycling, or swimming) helps reduce insulin resistance and maintain a healthy weight.
Stress management — yoga, mindfulness, and adequate sleep can support hormonal stability and mental well-being.
Medications — To manage hormones, regulate cycles, and reduce metabolic risks
Medication is chosen based on the individual’s symptoms, goals, and risk factors.
Hormonal birth control — combined oral contraceptives are the most commonly prescribed treatment for regulating periods, reducing acne, and controlling unwanted hair growth. Progestin-only pills, hormonal patches, or IUDs may also be considered.
Insulin-sensitising agents — metformin is often prescribed to improve insulin resistance, lower androgen levels, and promote more regular ovulation. It may also imrprove hyperandrogenic effects in some people.
Anti-androgens — medications like spironolactone may help with symptoms like hirsutism and acne. These are usually used alongside contraception due to the risk of birth defects.
Inositol supplements — myo-inositol and D-chiro-inositol are gaining popularity as over-the-counter supplements that may help improve insulin sensitivity, and menstrual regularity, though it is less effective than metformin.
Fertility treatments — For those trying to conceive
PCOS is a common cause of anovulatory infertility, but many women with PCOS can conceive with the right support.
Injectable hormones — gonadotropins may be used in monitored cycles if oral medications are ineffective.
Laparoscopic ovarian drilling — a minor surgical procedure used in select cases to trigger ovulation by reducing androgen-producing ovarian tissue.
Assisted reproductive technologies (ART) — IVF may be recommended if other methods are unsuccessful or if additional fertility issues are present.
Supportive therapies — For skin symptoms, emotional well-being, and long-term health
Managing PCOS often goes beyond hormone control and fertility.
Dermatological treatments — acne and hirsutism may be addressed with topical or oral treatments, laser hair removal, or electrolysis.
Mental health support — counselling, therapy, or medication may be helpful for depression, anxiety, or body image concerns.
Monitoring metabolic health — regular checks for blood pressure, cholesterol, glucose levels, and BMI are essential to prevent complications like diabetes and cardiovascular disease.
Effective PCOS management is long-term and often multi-faceted. With the right combination of lifestyle, medical, and emotional support, most women can control their symptoms, protect their health, and achieve their personal goals.
Summary
Polycystic Ovary Syndrome (PCOS) is a complex hormonal condition that affects many women of reproductive age in Singapore, often presenting with menstrual irregularities, acne, unwanted hair growth, weight challenges, and difficulties with fertility. While its exact cause remains unclear, PCOS is linked to genetic, hormonal, and lifestyle factors, particularly insulin resistance.
If left unmanaged, it can lead to long-term health issues such as type 2 diabetes, cardiovascular disease, and endometrial cancer. Diagnosis is based on a combination of symptoms, blood tests, and ultrasound findings, and treatment is tailored to each individual’s needs. Management options include lifestyle changes, medications to regulate hormones or improve insulin sensitivity, fertility treatments, and supportive therapies for mental health and skin-related concerns.
With early diagnosis and a structured treatment plan, most women can manage their symptoms and protect their long-term health. If you suspect you may have PCOS or are struggling with any of its effects, schedule a consultation with us to receive personalised, comprehensive care.
PCOD (polycystic ovary disease) refers to many immature follicles on the ovaries, mostly a descriptive ultrasound finding, whereas PCOS (polycystic ovary syndrome) is a broader metabolic and hormonal disorder involving multiple symptoms and health risks.
Yes, PCOS often runs in families. Having a close relative with PCOS increases your chances of developing it, reflecting underlying genetic factors in its development.
Untreated PCOS may lead to endometrial hyperplasia (excess uterine lining), which increases the risk of endometrial cancer. Regular menstrual regulation and follow-up reduce this risk.
PCOS is one of the most common causes of infertility due to the lack of egg release (anovulation). Women with PCOS also have a higher risk of complications during pregnancy, including gestational diabetes, preeclampsia, preterm birth, and miscarriage, but many still have successful pregnancies with appropriate care.
No, PCOS doesn’t disappear after menopause. Hormonal imbalance shifts, but metabolic complications like insulin resistance, heart disease, and risk of endometrial cancer can continue if not managed.
Yes, elevated androgens in PCOS can trigger androgenic alopecia, causing hair thinning on the scalp. It is often reversible with hormone balance restoration and targeted treatments.
Some women experience irregular cycles, acne, or hirsutism after stopping hormonal contraceptives—this transient pattern is often called post‑pill PCOS. It may resolve within 3–6 months as hormone levels rebalance.
chat with us
Welcome to The Metabolic Clinic
Holistic Care for Hormones, Bones, and Metabolic Health
Dr Dinesh graduated with honours from Monash University, Melbourne in 2009, receiving the Prince Henry's Prize in Surgery. During his endocrinology training in Melbourne, he won the top registrar award at the Endocrine Society of Australia Clinical Weekend in 2016, followed by securing Australia's only Andrology fellowship in 2017. Upon returning to Singapore, he was the sub-speciality lead for adrenal, pituitary, and bone services at Khoo Teck Puat Hospital and established The Metabolic Bone Clinic.
A passionate educator, he served as Associate Programme Director for Endocrinology at NHG, training the next generation of endocrinologists, and received the NHG Teaching Award for Senior Doctors in 2023. An expert endocrinologist with proficiency in both general and sub-speciality endocrinology, he has an interest in longevity through improving cardiovascular risk, metabolism, bone health, and muscle loss prevention, with the ultimate aim of improving the number of healthy years in one's life.
10+ Years of Experience in Hormone & Metabolic Health
Founder of The Metabolic Bone Clinic in Khoo Teck Puat Hospital
Sub-specialist training with international experts in Melbourne, Australia
Clinical Interest in Longevity & Metabolic Health
START YOUR PERSONALISED HEALTH JOURNEY
If you’re not achieving your treatment targets, struggling with weight changes, fatigue, or unexplained symptoms—it’s time to take a deeper look.
Get clarity with a tailored plan built around you and improving your metabolic health.