Abnormal adrenal growths that can be benign or functional, sometimes leading to high blood pressure, weight changes or hormonal shifts.
An adrenal gland tumour is an abnormal growth in one of the adrenal glands that may or may not produce excess hormones, leading to symptoms such as high blood pressure, fatigue, weight changes, through hormonal imbalance.
What is an adrenal gland tumour?
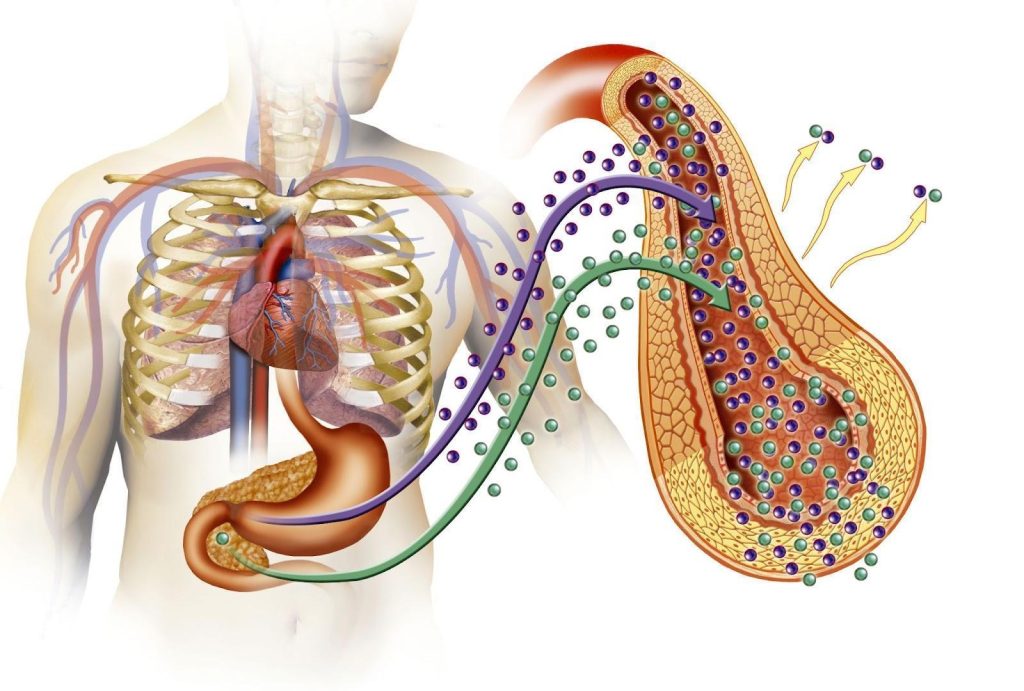
The adrenal glands are paired endocrine organs located above each kidney. Each gland consists of two distinct regions: the adrenal cortex, which produces steroid hormones such as cortisol and aldosterone, and the adrenal medulla, which secretes ‘fight or flight’ hormones like adrenaline and noradrenaline. These hormones play a central role in regulating blood pressure, metabolism, electrolyte balance, and the body’s acute stress response.
An adrenal gland tumour refers to any abnormal growth arising from the adrenal tissue. These tumours may be detected incidentally during imaging for unrelated conditions (an ‘incidentaloma’) or may come to attention due to hormonal symptoms or mass effect.
Adrenal tumours are classified based on their hormonal activity:
Non-functioning tumoursdo not secrete hormones and are often asymptomatic at the time of diagnosis. Many are benign and may require only monitoring.
Functioning tumours produce excess hormones independently of the body’s regulatory mechanisms. These can result in clinically significant hormonal syndromes and typically require targeted investigation and treatment.
Assessment of an adrenal mass involves determining its functional status, evaluating the risk of malignancy, and guiding appropriate management, which may range from observation and medication to surgical removal.
What are the common types of adrenal gland tumours?
Adrenal gland tumours are classified based on whether they secrete hormones and, if so, which hormones they produce. The three most clinically significant types of functioning adrenal tumours are:
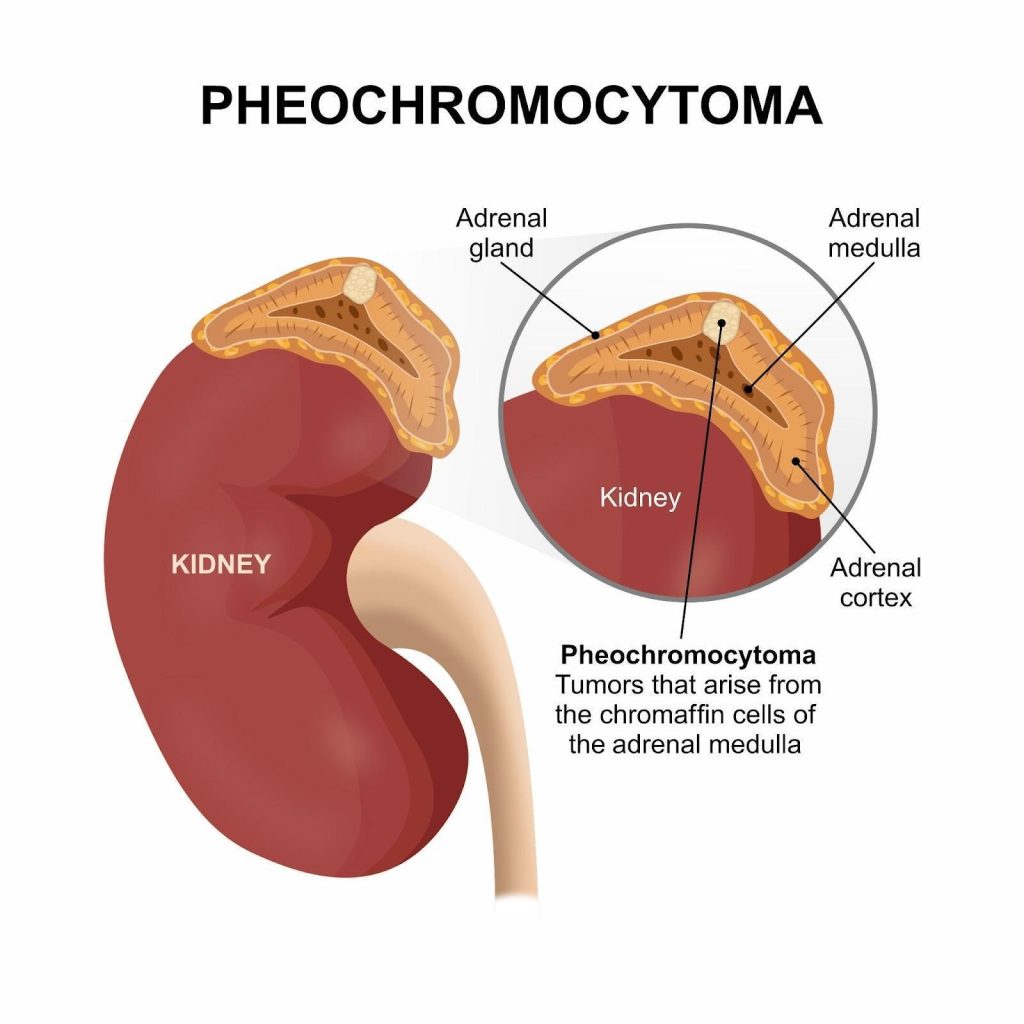
Phaeochromocytoma — Phaeochromocytomas arise from the chromaffin cells of the adrenal medulla and secrete excess catecholamines, primarily adrenaline and noradrenaline. This leads to symptoms such as persistent or episodic high blood pressure, headaches, palpitations, sweating, and anxiety. Although most are benign, they can be life-threatening if not recognised and managed appropriately, especially during physical stress or surgery. Dr. Dinesh has seen patients develop a blood pressure of 300mmHg before in phaeochromocytoma crisis. A small proportion may be malignant or part of inherited syndromes such as MEN2 or von Hippel–Lindau disease.
Primary hyperaldosteronism (Conn’s syndrome) — this condition typically results from an aldosterone-secreting adenoma in the adrenal cortex. Excess aldosterone causes the kidneys to retain sodium and excrete potassium, leading to high blood pressure and low blood potassium levels (hypokalaemia). Believe it or not, 5 to 15 percent of patients with hypertension may have primary hyperaldosteronism! It is underdiagnosed because symptoms can be subtle. Early identification is important as primary hyperaldosteronism markedly increases the risk of stroke, heart attack and kidney disease compared to normal hypertension (essential).
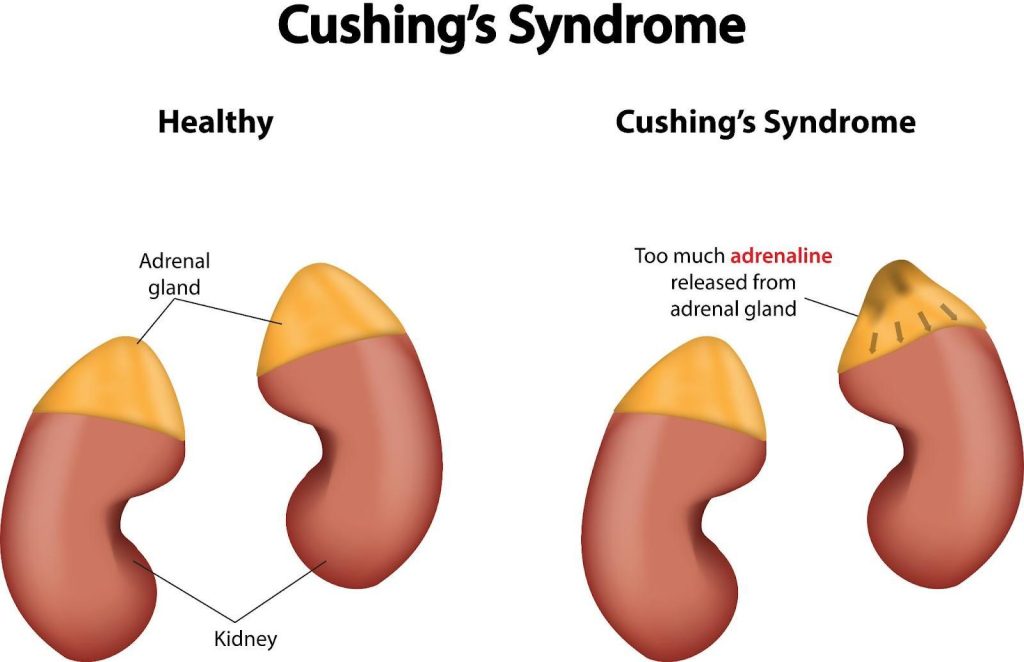
Cushing’s syndrome (adrenal cause) — when a tumour in the adrenal cortex produces excess cortisol, it leads to a form of Cushing’s syndrome that is independent of pituitary control. Clinical features include central weight gain, facial fullness (moon face), muscle weakness, thinning of the skin, easy bruising, and mood disturbances. Left untreated, cortisol excess can lead to serious complications such as diabetes, osteoporosis, and cardiovascular disease. Dr. Dinesh comments that this is a condition that needs to be ruled out if patients continuously gain weight.
Most of these tumours are benign adenomas, but a small number may be malignant. Accurate biochemical testing and imaging are essential to determine the functional status and nature of the tumour.
Pheochromocytoma is caused by abnormal growth of hormone-producing chromaffin cells, often due to sporadic changes or inherited genetic mutations.
What symptoms can adrenal gland tumours cause?
The symptoms vary depending on the type of hormone the tumour secretes. Below is a summary of key symptoms associated with the three main types of functioning adrenal tumours:
Tumour Type
Hormone Involved
Common Symptoms(Most frequent in bold)
Phaeochromocytoma
Adrenaline / Noradrenaline
Sudden or sustained high blood pressurePalpitationsExcessive sweatingHeadachesAnxiety or panic attacksTremors
High blood pressure (often resistant to treatment)Low potassium (hypokalaemia)Muscle cramps or weaknessFatigueIncreased thirst and urination
Cushing’s syndrome
Cortisol
Central weight gain (abdomen, face, upper back)Rounded face (“moon face”)Thin skin and easy bruisingPurple stretch marksMuscle weaknessMood changes (depression, irritability)Irregular periods or decreased libido
Non-functioning adrenal tumours, which do not secrete hormones, are usually asymptomatic and are often detected incidentally during imaging. However, if the tumour grows large, it may cause non-specific abdominal discomfort or pressure symptoms and occasionally bleeding into the tumor can occur (haemorrhage).
Cushing’s syndrome is caused by excess cortisol production, leading to weight gain, muscle weakness, thinning skin, and high blood pressure.
Who is at risk of an adrenal gland tumour in Singapore?
Most adrenal gland tumours arise without a clear cause, but certain groups are at higher risk than others. While many of these tumours are benign and non-functional, some are linked to hormone excess or inherited genetic conditions.
Age group most affected — adrenal tumours are most commonly diagnosed between the ages of 40 and 60. This is likely due to a large number of them being diagnosed incidentally on CT scans for other conditions in this age group according to Dr. Dinesh. However, functioning tumours like phaeochromocytoma may appear earlier, particularly in those with genetic syndromes.
Genetic testing and regular surveillance may be advised for those in high-risk families.
Unexplained, early or resistant hypertension — persistent high blood pressure, especially if difficult to control or associated with low potassium levels, may suggest an underlying functional adrenal tumour such as primary hyperaldosteronism or phaeochromocytoma. Having an early diagnosis of hypertension before the age of 40, needs to be investigated to rule this out.
History of malignancy — in patients with known cancers, particularly of the lung, breast, kidney, or melanoma, the adrenal gland can be a site of metastasis. Any adrenal mass in these individuals warrants careful evaluation. Dr. Dinesh says, this is why CT scans of the lungs include the adrenals which are lower down, to rule out metastases there.
Early identification of risk factors, particularly in symptomatic individuals or those with a relevant family history, can lead to timely diagnosis and treatment of adrenal tumours before complications arise.
Are adrenal tumours cancerous?
Most adrenal tumours are benign and do not pose a threat of cancer. However, a small proportion may be malignant, either arising from the adrenal gland itself or representing metastases from cancers elsewhere in the body.
Benign adrenal tumours — the majority of adrenal tumours are non-cancerous adenomas. These may be either non-functioning or hormone-secreting. While they can still cause health issues due to excess hormone production, they do not spread to other organs.
Adrenocortical carcinoma — this is a rare but aggressive cancer arising from the adrenal cortex. It may present with signs of hormone excess including masculinsation in women, symptoms due to mass effect, or be discovered incidentally. These tumours often exceed 4 cm in size and may invade surrounding tissues or spread to distant organs.
Metastatic adrenal tumours — the adrenal glands are a common site for metastasis from cancers such as lung, breast, kidney, and melanoma. In patients with a history of malignancy, an adrenal mass requires careful assessment to distinguish primary adrenal pathology from secondary involvement.
Suspicious features on imaging — large tumour size (especially >4 cm), irregular margins, rapid growth, and high unenhanced CT density may raise concern for malignancy. Further evaluation or surgical removal may be warranted in such cases.
Determining whether an adrenal tumour is malignant relies on a combination of imaging characteristics, hormone testing, and, in some cases, histopathological examination after surgery.
How are adrenal gland tumours diagnosed?
Diagnosing an adrenal gland tumour involves determining two key factors: whether the tumour is producing hormones, and whether it shows any features suspicious for cancer. The process typically combines hormone testing with imaging studies.
Hormonal assessment — blood and urine tests are used to detect excess hormone production. These may include:
Cortisol levels via low-dose dexamethasone suppression test, late-night salivary cortisol, or 24-hour urinary cortisol to check for Cushing’s syndrome
Imaging investigations — CT (computed tomography) or MRI (magnetic resonance imaging) scans of the abdomen are typically performed to locate and characterise the adrenal mass. Radiological features such as size, shape, density, and contrast washout help distinguish benign from potentially malignant lesions.
Adrenal vein sampling — in selected cases, particularly when primary hyperaldosteronism is suspected, a specialised procedure called adrenal vein sampling may be needed. This test helps determine which gland is overproducing aldosterone and guides surgical decision-making.
Nuclear medicine scans — in certain cases, functional imaging such as Dotatate scans may be used to evaluate suspected phaeochromocytoma or to assess for metastases.
Accurate diagnosis is essential to guide treatment. A multidisciplinary approach involving endocrinology, radiology, and sometimes surgery ensures that functional tumours are managed appropriately, and non-functional ones are monitored safely.
What are the treatment options for adrenal gland tumours?
Treatment depends on several factors, including the tumour’s size, whether it is producing hormones, and any suspicion of malignancy. The goal is to manage hormone excess when present and to remove or monitor the tumour appropriately.
Surgical removal — adrenalectomy, or surgical removal of the affected adrenal gland, is the treatment of choice for most functioning tumours and for any lesion suspicious for cancer. Laparoscopic (keyhole) surgery is commonly used for smaller, localised tumours, while larger or invasive tumours may require open surgery.
Pre-operative medical management — for hormone-secreting tumours, stabilisation before surgery is essential.
Medical therapy — when surgery is not possible, or in cases where hormone control is needed before or after surgery, medications may be used to block or suppress excess hormone production.
Monitoring — non-functioning tumours that are small (typically less than 4 cm), stable, and show benign features on imaging may not require immediate treatment. These are often monitored over time with repeat imaging and hormone testing.
Treatment for adrenal cancer — adrenocortical carcinoma is rare but aggressive. Treatment involves surgical resection when feasible, often followed by mitotane (an adrenolytic drug), and sometimes chemotherapy or radiotherapy. Long-term follow-up is essential due to high recurrence risk.
A tailored treatment plan, guided by endocrine testing, imaging findings, and individual patient factors, is essential to ensure optimal outcomes.
Summary
Adrenal gland tumours are growths that arise within the adrenal glands and may or may not produce excess hormones. Some are silent while others can lead to significant health problems by disrupting hormone balance, causing symptoms such as high blood pressure, fatigue, weight changes, and electrolyte disturbances. An endocrinologist is essential in triaging and managing these tumours.
Common functional tumours include phaeochromocytoma, primary hyperaldosteronism, and cortisol-secreting tumours linked to Cushing’s syndrome. Diagnosis involves a combination of hormonal testing and imaging, and treatment is tailored based on tumour type, size, and function. With timely evaluation and appropriate management, most patients achieve good outcomes.
If you have symptoms suggestive of a hormone imbalance or have been diagnosed with an adrenal mass, schedule a consultation with The Metabolic Clinic for a comprehensive assessment and personalised care plan.
Adrenal gland tumours may remain stable without treatment, but they do not typically shrink on their own. Regular monitoring is recommended to detect any changes.
Doctors typically investigate adrenal gland tumours through a combination of hormone blood/urine tests and imaging scans like CT or MRI. These help assess both function and structure.
Most adrenal gland tumours do not cause pain. However, in rare cases where the tumour is large, bleeding or pressing on nearby structures, patients may feel vague discomfort or fullness in the abdomen.
Growth rates vary. Benign adrenal gland tumours often grow slowly or remain stable, while malignant ones may enlarge rapidly and require urgent evaluation.
No, not all adrenal gland tumours are functional. Many are non-secreting and cause no hormonal symptoms, which is why they are often found incidentally on imaging.
There are no known lifestyle measures that can prevent an adrenal gland tumour. However, managing overall health, blood pressure, and seeking evaluation for unexplained symptoms may aid early detection.
Surgery is recommended for hormone-producing tumours or those with suspicious imaging features. Small, non-functioning adrenal gland tumours may be monitored without immediate intervention.
Chronic stress may indirectly influence adrenal hormone activity but is not a proven direct cause of an adrenal gland tumour. Most tumours develop due to sporadic cellular changes or, less commonly, genetic conditions.
chat with us
Welcome to The Metabolic Clinic
Holistic Care for Hormones, Bones, and Metabolic Health
Dr Dinesh graduated with honours from Monash University, Melbourne in 2009, receiving the Prince Henry's Prize in Surgery. During his endocrinology training in Melbourne, he won the top registrar award at the Endocrine Society of Australia Clinical Weekend in 2016, followed by securing Australia's only Andrology fellowship in 2017. Upon returning to Singapore, he was the sub-speciality lead for adrenal, pituitary, and bone services at Khoo Teck Puat Hospital and established The Metabolic Bone Clinic.
A passionate educator, he served as Associate Programme Director for Endocrinology at NHG, training the next generation of endocrinologists, and received the NHG Teaching Award for Senior Doctors in 2023. An expert endocrinologist with proficiency in both general and sub-speciality endocrinology, he has an interest in longevity through improving cardiovascular risk, metabolism, bone health, and muscle loss prevention, with the ultimate aim of improving the number of healthy years in one's life.
10+ Years of Experience in Hormone & Metabolic Health
Founder of The Metabolic Bone Clinic in Khoo Teck Puat Hospital
Sub-specialist training with international experts in Melbourne, Australia
Clinical Interest in Longevity & Metabolic Health
START YOUR PERSONALISED HEALTH JOURNEY
If you’re not achieving your treatment targets, struggling with weight changes, fatigue, or unexplained symptoms—it’s time to take a deeper look.
Get clarity with a tailored plan built around you and improving your metabolic health.