A condition caused by prolonged cortisol elevation, commonly associated with steroid medications or hormonal imbalances.
What is Cushing syndrome?
Cushing syndrome, also known as hypercortisolism, is a disorder caused by prolonged exposure to high levels of cortisol in the body. Cortisol is a steroid hormone produced by the adrenal glands that plays a vital role in regulating metabolism, blood pressure, the body’s response to stress and immune function. While short-term increases in cortisol are part of the normal stress response, persistently raised levels can lead to significant health problems.
Cushing syndrome is relatively rare but serious. It can cause a wide range of symptoms, including weight gain (particularly around the face, neck, and abdomen), thinning of the skin, muscle weakness, high blood pressure, diabetes, osteoporosis, recurrent infections and mood changes. Because many of these symptoms develop gradually and overlap with more common conditions, diagnosis can be challenging. Early recognition and treatment are important to prevent complications and restore hormonal balance.
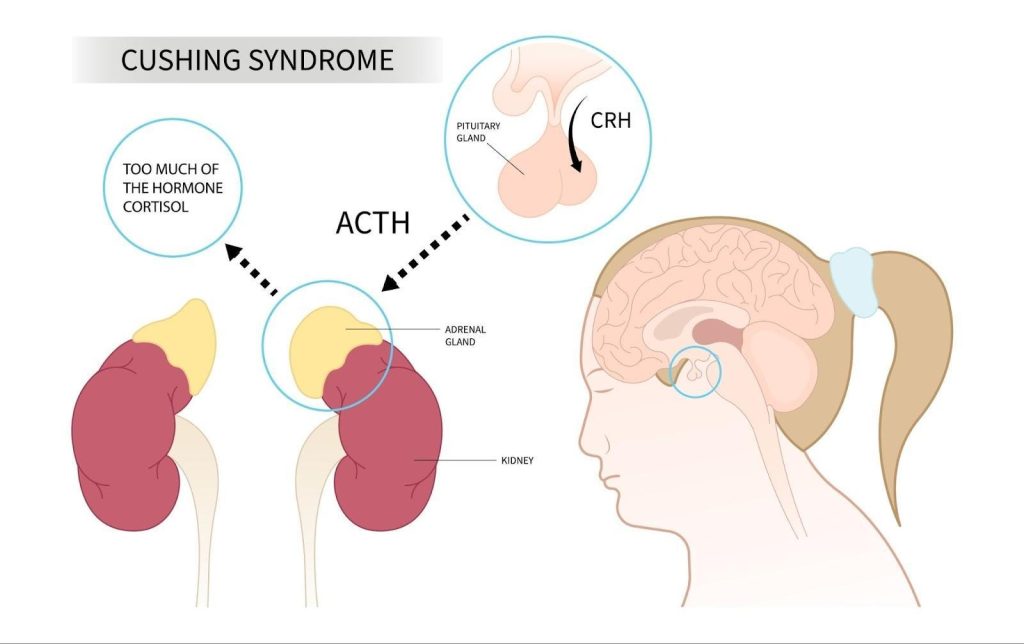
Cushing syndrome is a rare hormonal disorder caused by prolonged exposure to excess cortisol, most commonly due to excess ACTH secretion from the pituitary gland in the brain.
What causes Cushing syndrome?
Cushing syndrome develops when the body is exposed to persistently high levels of cortisol, either from within the body (endogenous causes) or from outside sources (exogenous causes).
Endogenous causesarise when the body produces too much cortisol on its own. The most common reason is a pituitary gland tumour, usually benign, that releases excessive adrenocorticotropic hormone (ACTH). This condition is referred to as Cushing’s disease. In other cases, tumours in the adrenal glands themselves can produce cortisol directly, without ACTH stimulation. Less commonly, tumours in other parts of the body, such as the lungs or pancreas may produce ACTH, a phenomenon known as ectopic ACTH production.
Exogenous causesare linked to medical treatment. Long-term use of glucocorticoid medications, which are prescribed to control inflammation in conditions like asthma, lupus, rheumatoid arthritis or to prevent organ rejection after transplant, can mimic the effects of excess cortisol. In Singapore, as mentioned earlier, TCM laced with the steroid dexamethasone or similar is a common cause. This is the most frequent cause of Cushing syndrome in clinical practice but is decreasing in incidence with increased regulation
The underlying cause determines both the treatment approach and the long-term outlook. Identifying whether excess cortisol is medication-related, pituitary-driven, adrenal in origin or due to ectopic ACTH is essential for accurate management. In any event, most cases are curable.
What is the difference between Cushing’s syndrome and Cushing disease?
Although the two terms are often used interchangeably, they describe different conditions.
Cushing syndrome refers to the overall clinical picture of prolonged exposure to high levels of cortisol, regardless of the cause. This includes cases due to long-term glucocorticoid steroid use, adrenal tumours, ectopic ACTH production or pituitary disease.
Cushing disease, on the other hand, is a specific form of Cushing syndrome caused by a benign pituitary adenoma that produces excessive amounts of adrenocorticotropic hormone (ACTH). ACTH is the hormone that controls cortisol production from the adrenal glands. This overstimulation drives the adrenal glands to release excess cortisol.
In short, Cushing disease is a subset of Cushing syndrome. Identifying the distinction is important, as the underlying cause determines the most suitable treatment approach.
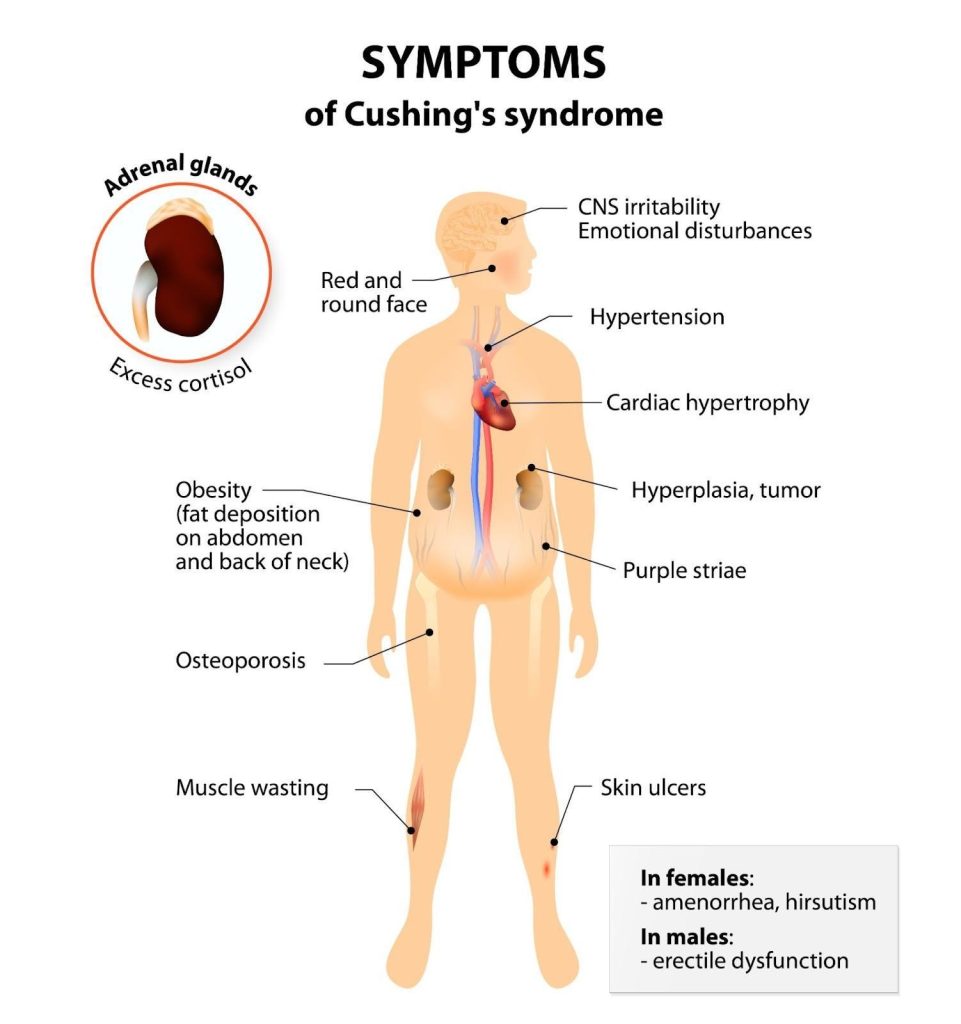
What are the symptoms of Cushing syndrome?
The symptoms of Cushing syndrome develop gradually and can vary depending on the underlying cause, the severity of cortisol excess and how long the condition has been present. Many signs are non-specific, which makes diagnosis challenging, as they may be mistaken for more common health issues like insulin resistance from obesity.
One of the hallmark features is weight gain, particularly around the abdomen, face and upper back, leading to a rounded “moon face” and a fatty hump between the shoulders (“buffalo hump” – more appropriately named dorsocervical fat pad). The arms and legs, however, often remain relatively slender due to muscle wasting.
Violaceous striae are purplish stretch marks typically seen in Cushing syndrome due to prolonged cortisol excess causing thinning of the skin and loss of collagen support.
Other common features include:
Skin changes — thinning of the skin, easy bruising, slow wound healing and the appearance of wide, purple stretch marks (striae), especially on the abdomen, thighs and breasts. Dr. Dinesh says this is highly specific for this condition and differentiates simple obesity from a case that is suspicious of Cushing’s.
Muscle and bone effects — progressive muscle weakness, fatigue and increased risk of fractures.
Cushing syndrome can cause symptoms such as weight gain, thinning skin, muscle weakness, high blood pressure, mood disturbances and reproductive issues including irregular periods in women and reduced libido or erectile dysfunction in men.
What are the complications of Cushing syndrome?
If left untreated, Cushing syndrome can lead to serious and sometimes life-threatening complications due to the prolonged effects of excess cortisol on the body.
Cardiovascular complications are among the most significant. People with Cushing syndrome are at increased risk of high blood pressure, heart disease and stroke. Cortisol also contributes to central obesity, high cholesterol and diabetes, all of which further strain the cardiovascular system.
Bone and muscle problems are common. Persistent cortisol excess weakens bone by causing increased bone loss, making osteoporosis and fractures more likely, particularly in the spine, hips and ribs. Muscle wasting can impair mobility and reduce overall strength.
Infections may occur more frequently, as cortisol suppresses the immune system, leaving the body more vulnerable to bacterial, viral and fungal illnesses.
In women, reproductive complications like infertility or irregular menstrual cycles may persist, while in men, low testosterone can result in reduced libido and erectile dysfunction. Over time, untreated Cushing syndrome significantly reduces quality of life and can shorten life expectancy.
Who is at risk of Cushing syndrome in Singapore?
Cushing syndrome is uncommon, but certain groups of people face a higher likelihood of developing it.
Glucocorticoid use — the leading risk factor is long-term use of glucocorticoid medicines, particularly at high doses or unknowingly for those on traditional Chinese medicine laced with glucocorticoids. These drugs are often prescribed for conditions like asthma, rheumatoid arthritis, lupus, inflammatory bowel disease or after organ transplantation. In TCM it is used in concoctions for arthritis/ joint pains. Sometimes patient’s obtain these from overseas. Prolonged exposure to synthetic steroids can mimic the effects of excess cortisol in the body.
Pituitary or adrenal tumours — benign growths in the pituitary gland or adrenal glands can interfere with normal hormonal control, causing overproduction of adrenocorticotropic hormone (ACTH) or cortisol respectfully. Less commonly, cancers outside these glands, including those in the lungs or pancreas, may produce ACTH and trigger the condition.
Other considerations — while lifestyle alone does not directly cause Cushing syndrome, personal medical history and awareness of long-term steroid use are important in identifying those at risk. Early recognition allows for timely evaluation and treatment, reducing the risk of complications.
Can Cushing syndrome be prevented?
Because many cases of Cushing syndrome are caused by tumours of the pituitary or adrenal glands or by ectopic ACTH production, the condition cannot always be prevented. However, certain steps can reduce the likelihood of developing cortisol excess linked to medical treatment.
Careful use of glucocorticoids — the most effective preventive strategy is the cautious use of glucocorticoid steroid medicines. Doctors prescribe the lowest effective dose for the shortest possible time, and patients are advised not to stop or adjust their medication without medical supervision. Regular monitoring helps detect early signs of excess cortisol before complications develop.
Awareness of symptoms — people who require long-term steroid therapy should be aware of the potential side effects, such as weight gain, skin changes or mood disturbances, and report these promptly to their healthcare provider.
Ongoing follow-up — for individuals with known pituitary or adrenal abnormalities, regular follow-up with an endocrinologist allows early intervention if hormone levels rise again or if tumours recur.
While Cushing syndrome cannot always be avoided, early detection and proactive medical care play a crucial role in reducing its impact and improving long-term outcomes.
How is Cushing syndrome diagnosed?
Diagnosing Cushing syndrome can be challenging because many of its symptoms, such as weight gain, fatigue and mood changes, overlap with more common health conditions. A stepwise approach combining clinical assessment, laboratory testing and imaging studies is usually required.
Medical history and examination — the process begins with a detailed review of symptoms, medical history and any use of glucocorticoid medications. A physical examination may reveal typical features, such as central obesity, thinning of the skin and purple stretch marks.
Hormone measurements — additional blood tests measure levels of adrenocorticotropic hormone (ACTH) to identify whether excess cortisol is driven by pituitary stimulation, adrenal overproduction or ectopic ACTH production from a tumour elsewhere in the body.
Imaging studies — once abnormal hormone production is confirmed, imaging such as MRI scans of the pituitary gland or CT scans of the adrenal glands may be performed to locate the source of the problem. In some cases, specialised procedures, such as sampling blood from veins near the pituitary, are needed to pinpoint the cause.
Accurate diagnosis is essential, as the treatment strategy depends entirely on whether the syndrome is due to medication use, a pituitary tumour, an adrenal tumour or ectopic ACTH production.
What are the treatment options for Cushing syndrome in Singapore?
Treatment aims to reduce cortisol levels to normal, relieve symptoms and prevent long-term complications. The approach depends on the underlying cause of the condition.
Medication-related cases — when Cushing syndrome results from long-term glucocorticoid use, doctors usually aim to gradually reduce the dose or switch to alternative therapies. This must be done carefully under medical supervision of the relevant specialist, as sudden withdrawal can cause adrenal insufficiency.
Pituitary tumours — for Cushing’s disease caused by a pituitary adenoma, surgery to remove the tumour is usually the most preferable treatment method. If surgery is not fully effective or feasible, radiotherapy or medicines that lower cortisol production may be recommended.
Adrenal tumours — adrenal gland tumours producing excess cortisol are generally treated with surgical removal. In cases where surgery is not an option, medications that block cortisol production may be prescribed.
Ectopic ACTH-producing tumours — when tumours in the lungs, pancreas or other organs cause excess ACTH, treatment focuses on removing or controlling the primary tumour. This may involve surgery, chemotherapy or radiotherapy, depending on the type and stage of the tumour.
Medicines — several drug therapies, such as ketoconazole, can be used to reduce cortisol levels if surgery is not possible or while awaiting definitive treatment. This is always the second or third line due to the side effects of the medication.
Treatment often requires a multidisciplinary team involving endocrinologists, surgeons, radiologists and sometimes oncologists. Regular monitoring after treatment is important, as hormone balance can take time to stabilise and recurrence is possible.
Prognosis and recovery in Cushing syndrome
The outlook for people with Cushing syndrome depends on the cause, the severity of cortisol excess and how early treatment begins. With timely diagnosis and appropriate management, many patients experience significant improvement and may return to good health, though recovery can take months to years.
After surgery — successful removal of a pituitary or adrenal tumour often leads to normalisation of cortisol levels. However, the adrenal glands may take time to resume normal function, and temporary cortisol replacement therapy is sometimes required. Long-term follow-up is essential, as tumours can occasionally recur.
Medication-related cases — when caused by glucocorticoid treatment, gradual reduction of the medication usually leads to recovery, although this process must be carefully managed to avoid adrenal insufficiency. Some patients may continue to require low-dose steroids for their underlying condition.
Residual effects — even after successful treatment, some complications of Cushing syndrome may persist. Osteoporosis, diabetes, high blood pressure or mood disorders may require ongoing management. Muscle weakness and fatigue can take time to improve, and patients often benefit from physiotherapy and lifestyle support.
Overall outlook — with appropriate treatment, many individuals achieve good long-term outcomes, though quality of life may be affected if complications have already developed. Early recognition of the syndrome offers the best chance of full recovery and prevention of lasting health problems.
Summary
Cushing syndrome, also known as hypercortisolism, is a rare but serious condition caused by prolonged exposure to excess cortisol. It can arise from long-term glucocorticoid use, pituitary or adrenal tumours or less commonly, tumours in other parts of the body producing ACTH. The syndrome presents with a wide range of symptoms, including weight gain, skin changes, muscle weakness, high blood pressure and mood disturbances, and may lead to serious complications if left untreated.
Diagnosis requires a careful combination of clinical assessment, laboratory tests and imaging, while treatment depends on the underlying cause, ranging from medication adjustments to surgery or targeted therapies. With timely recognition and management, many patients can achieve good recovery, though ongoing care is often needed to manage residual effects.
If you are concerned about symptoms of excess cortisol or have been advised to undergo evaluation for Cushing syndrome, schedule a consultation with The Metabolic Clinic for expert diagnosis, personalised treatment, and long-term care.
Some people with Cushing syndrome experience shortness of breath. This is usually due to weight gain around the chest and abdomen, muscle weakness or associated conditions such as high blood pressure, heart disease or an increased risk of blood clots in the lungs.
Yes, prolonged exposure to excess cortisol weakens bones, increasing the risk of osteoporosis and fractures, particularly in the spine, hips and ribs. This is one of the most common long-term complications.
In severe cases, excess cortisol can mimic the effects of another hormone called aldosterone, leading to increased loss of potassium in urine. This can result in hypokalaemia, which may cause muscle weakness, fatigue or heart rhythm disturbances.
Most cases of Cushing syndrome are not genetic and occur sporadically. However, very rarely, inherited conditions such as multiple endocrine neoplasia type 1 (MEN1) or Carney complex can predispose to tumours that lead to cortisol excess.
Yes, if untreated, Cushing syndrome can be fatal. The main risks come from cardiovascular complications such as heart attack, stroke and blood clots, as well as severe infections and uncontrolled diabetes or hypertension.
Many patients experience mood swings, irritability, anxiety or depression. Some also report memory difficulties or reduced concentration. Psychological support is often an important part of treatment.
Yes, excess cortisol raises blood glucose levels and can lead to type 2 diabetes or worsen existing diabetes. This may improve after successful treatment, but some people require long-term management.
High blood pressure is a common feature of Cushing syndrome and contributes to long-term cardiovascular risk. Controlling cortisol excess usually improves blood pressure, although some patients need ongoing treatment.
Yes, women may experience irregular or absent periods, while men may have reduced testosterone and erectile dysfunction. Both sexes may have reduced fertility, which can improve once cortisol levels are corrected.
Thinning of the skin, easy bruising, slow healing and purple stretch marks are characteristic. Acne and excess facial or body hair (especially in women) may also occur.
Yes, in children, growth retardation is often the first sign. Unlike adults, children may not show the typical redistribution of fat, making diagnosis more challenging.
Not always. Treatment depends on the cause: surgery may be needed for pituitary or adrenal tumours, but if it results from long-term glucocorticoid use, adjusting or reducing the medication may be sufficient under medical guidance.
chat with us
Welcome to The Metabolic Clinic
Holistic Care for Hormones, Bones, and Metabolic Health
Dr Dinesh graduated with honours from Monash University, Melbourne in 2009, receiving the Prince Henry's Prize in Surgery. During his endocrinology training in Melbourne, he won the top registrar award at the Endocrine Society of Australia Clinical Weekend in 2016, followed by securing Australia's only Andrology fellowship in 2017. Upon returning to Singapore, he was the sub-speciality lead for adrenal, pituitary, and bone services at Khoo Teck Puat Hospital and established The Metabolic Bone Clinic.
A passionate educator, he served as Associate Programme Director for Endocrinology at NHG, training the next generation of endocrinologists, and received the NHG Teaching Award for Senior Doctors in 2023. An expert endocrinologist with proficiency in both general and sub-speciality endocrinology, he has an interest in longevity through improving cardiovascular risk, metabolism, bone health, and muscle loss prevention, with the ultimate aim of improving the number of healthy years in one's life.
10+ Years of Experience in Hormone & Metabolic Health
Founder of The Metabolic Bone Clinic in Khoo Teck Puat Hospital
Sub-specialist training with international experts in Melbourne, Australia
Clinical Interest in Longevity & Metabolic Health
START YOUR PERSONALISED HEALTH JOURNEY
If you’re not achieving your treatment targets, struggling with weight changes, fatigue, or unexplained symptoms—it’s time to take a deeper look.
Get clarity with a tailored plan built around you and improving your metabolic health.