Bone Building Therapy (Anabolic Therapy for Osteoporosis)
A treatment approach that stimulates new bone formation, supporting stronger bone density in individuals with osteoporosis or high fracture risk.
Picture a morning stroll in a familiar park, until a stumble ends in a painful fracture. It sounds unlikely, but for hundreds in Singapore each year, this scenario is all too real. Hip fractures here have shot up dramatically — fivefold in women and 1.5 times in men since the 1960s.
Even more alarming, between 2017 and 2035, osteoporotic fractures in Singapore are predicted to climb by nearly 60%, from around 15,300 to over 24,100 cases annually. That’s tens of thousands of lives at stake. Tragically, these broken bones aren’t just painful, they are life-altering. One in five hip fracture victims dies within a year; and 40 to 60 percent face permanent loss of mobility and independence. 1 in 5 require either a helper or have to be institutionalised (loss of independence). These aren’t distant statistics, they are stories of parents, friends, and neighbours whose days of gardening, dancing, even simply bending down become impossible. And yet, osteoporosis remains underdiagnosed and underappreciated. A silent disease with disastrous consequences. While a DEXA scan might just show “low bone density,” it often fails to mirror the quiet dismantling of someone’s confidence and capability after a fracture.
Contrary to popular belief, osteoporosis is commonly managed by endocrinologists. This is because osteoporosis is fundamentally a metabolic bone disease, and hormone specialists can address the root cause of bone loss, often related to hormonal imbalances, such as declining oestrogen and testosterone levels. One such prescribed treatment is Anabolic Therapy, or Bone Building Therapy, which utilises bone-building agents to actively stimulate new bone formation rather than simply slowing bone loss.
What is Osteoporosis?
Osteoporosis is a chronic condition characterised by reduced bone density and deterioration of bone microarchitecture, which increases the risk of fractures, even from low-impact events. These fractures are not only painful but can also be disabling, often resulting in long-term loss of independence and a decline in overall quality of life.
While often associated with ageing or calcium deficiency, osteoporosis is fundamentally a hormone-driven condition, influenced by changes in key regulators of bone metabolism such as oestrogen and testosterone. These hormonal shifts disrupt the natural balance between bone formation and bone resorption, tipping the scale toward bone loss.
Bone is a highly functional, metabolic organ full of cells. Bone formation led by osteoblasts (bone-producing cells) must be the same as bone destruction by osteoclasts (bone-resorbing cells) in order for bone mass to be neutral. After menopause and in other disease states and with ageing, osteoclasts break more bone down than osteoblasts build and this results in the loss of bone density and bone fragility.
Although osteoporosis can affect anyone, it is most common in postmenopausal women, due to the sharp decline in oestrogen levels that occurs during menopause. Men may also develop osteoporosis, but more often than not, for men there is a disease process (secondary cause) that is causing it
Osteoporosis is broadly classified into primary and secondary forms:
Primary Osteoporosis
This is the most common form and is typically associated with age-related hormonal changes. It can only be diagnosed after secondary causes of osteoporosis have been ruled out (highlighted below). The most common cause is postmenopausal oestrogen loss in women but ageing also contributes such that 50 percent of those over the age of 80 have osteoporosis.
Secondary Osteoporosis
This type arises from identifiable medical conditions, medications, or other external factors that impair bone remodelling (the balance between bone formation and bone resorption/loss).
Common causes include:
Medications —long-term use of glucocorticoids, anti-epileptics, certain antidepressants, and chemotherapy agents can interfere with bone metabolism, leading to increased resorption and structural weakness.
Malabsorption syndromes — disorders like inflammatory bowel disease (IBD), celiac disease, anorexia nervosa, and patients who have undergone bariatric surgery may have impaired absorption of calcium and other nutrients vital for bone health.
Organ transplants — the long-term use of immunosuppressive therapies following transplant surgery can disrupt bone turnover and contribute to bone loss.
Chronic illnesses — diseases such as chronic kidney disease, HIV, cancers such as multiple myeloma, rheumatoid arthritis, cystic fibrosis, and inherited conditions like thalassaemia are also linked to increased bone fragility.
Alcohol abuse- Patients with cirrhosis and alcohol abuse have a combination of poor nutrition and direct toxicity on the bone from the alcohol resulting in lower bone mass.
Treatment and Management
Managing osteoporosis requires a combination of lifestyle modifications and medical therapy. Preventing falls through strength training, balance exercises, and maintaining physical activity is essential. Adequate nutrition, including sufficient calcium, vitamin D, and protein intake, is also critical for bone maintenance.
Pharmacological treatments fall into two major categories:
Antiresorptive agents, such as bisphosphonates, hormone replacement therapy (partially anabolic) (HRT), selective oestrogen receptor modulators (SERMs), calcitonin, and certain monoclonal antibodies (Denosumab), work by reducing bone resorption and slowing the progression of bone loss.
Anabolic agents, which include therapies like teriparatide and romosozumab, actively stimulate new bone formation and are typically recommended for patients at high risk of fracture.
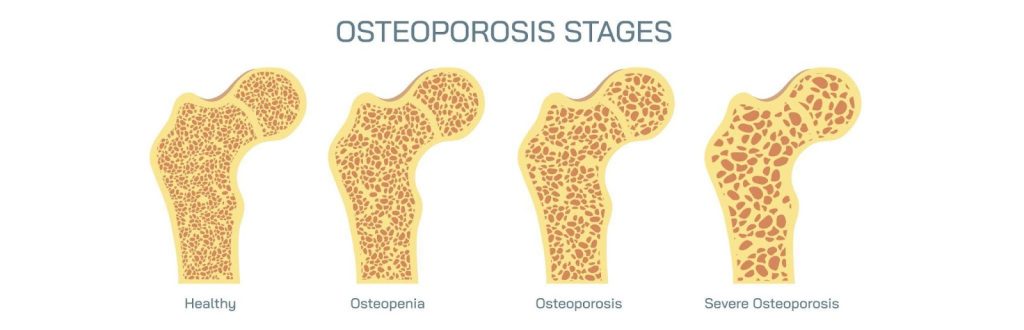
Osteoporosis can cause the bones to become increasingly weak and porous, progressing from osteopenia to osteoporosis and eventually to severe osteoporosis, where the risk of fractures is significantly heightened.
For decades, the cornerstone of osteoporosis management has relied on antiresorptive medications, treatments designed to slow down the rate at which bone is broken down. These include bisphosphonates, selective oestrogen receptor modulators (SERMs) such as raloxifene, and monoclonal antibodies like denosumab. While these therapies have proven highly-effective in stabilising bone density and reducing fracture risk in many patients, they have been superseded by anabolic (bone-building therapy) in efficacy for those at high risk of fractures. .
Anti-resorptives work by reducing bone resorption, helping to preserve existing bone. However, they do not actively stimulate the formation of new bone. For patients with a higher risk of fracture, their ability to reduce fractures may not be sufficient. Over time, the ability of most of these medications to significantly improve bone strength plateaus, and in some cases, patients may continue to fracture despite long-term therapy if bone mineral density was very low to start with.
This is where anabolic (bone-building) therapy represents a major advancement. Unlike antiresorptive treatments, anabolic agents directly stimulate osteoblast activity—the cells responsible for forming new bone—resulting in the best improvements in bone mass, strength, and structural integrity. They have been proven in trials to reduce fracture risk the most and improve bone mineral density more than anti-resorptive medications.
Bone-building therapy is particularly crucial for:
Patients who have sustained multiple low-impact fractures, including hip or vertebral fractures.
Individuals with a T-score ≤ –3.0, indicating severe bone loss.
Those who have had suboptimal response or intolerance to antiresorptive agents.
Patients identified as very high fracture risk based on clinical factors or fracture risk assessment tools (such as FRAX).
Several large-scale clinical trials have shown that anabolic therapies like teriparatide and romosozumab can reduce vertebral and non-vertebral fractures by up to 80%. These outcomes are especially significant in the first year of treatment, offering rapid protection for the most vulnerable patients.
Moreover, anabolic therapy is typically followed by antiresorptive treatment to consolidate gains and maintain newly formed bone. This sequential strategy has been shown to be more effective than either approach alone in reducing long-term fracture risk. In fact anabolic therapy must be started first prior to an anti-resorptive where possible as using it as a ‘second-line’ impairs its ability to cause the greatest improvement in bone mineral density.
In the context of Singapore’s ageing population and rising rates of osteoporotic fractures, bone-building therapy offers a vital opportunity to not only prevent injury but to restore confidence, mobility, and quality of life. For patients at high risk, it may be the difference between managing osteoporosis and overcoming it.
What is Bone-Building (Anabolic) Therapy?
Bone-building therapy, medically known as anabolic therapy, is a specialised form of osteoporosis treatment designed to stimulate the formation of new bone tissue. Unlike traditional antiresorptive medications, which slow the breakdown of bone, anabolic therapies actively enhance bone formation, offering a crucial therapeutic option for individuals at high risk of fractures or those who have not responded adequately to conventional treatments.
Anabolic therapy works by directly targeting the function of osteoblasts, the cells responsible for bone synthesis. In healthy bone remodelling, osteoblasts build bone while osteoclasts break it down. In osteoporosis, this balance is disrupted — resorption outpaces formation, leading to bone loss. Anabolic agents shift this balance by promoting osteoblast activity, increasing bone mass, and improving the architecture of both trabecular and cortical bone.
There are currently two main anabolic agents approved for the treatment of osteoporosis:
Teriparatide – a synthetic form of the first 34 amino acids of human parathyroid hormone (PTH 1-34). Administered as a daily subcutaneous injection, teriparatide stimulates bone formation by mimicking the natural action of intermittent PTH exposure, which preferentially activates osteoblasts over osteoclasts. It has been shown to significantly increase bone mineral density (BMD) in the spine and hip and reduce the risk of both vertebral and non-vertebral fractures. It is also the only therapy that is safe for those who have had a rare side-effect of anti-resorptives – The atypical femoral fracture
Romosozumab – a monoclonal antibody that targets sclerostin, a protein that inhibits bone formation. By blocking sclerostin, romosozumab enhances osteoblast activity while simultaneously reducing bone resorption—a unique dual mechanism of action. It is administered as a monthly injection over 12 months and has demonstrated rapid and significant increases in BMD, particularly in patients with severe osteoporosis and recent fractures. It is the gold-standard in osteoporosis treatment having the best outcomes in trials. One year of romosuzumab therapy is equivalent to 5 years of denousmab treatment in trials.
The primary indication for anabolic therapy is in patients with severe osteoporosis or very high fracture risk. This includes individuals with multiple fragility fractures, those with extremely low BMD, or patients who have failed or cannot tolerate antiresorptive medications.
Anabolic therapy is typically prescribed as a limited-duration treatment, usually for 12 to 24 months, due to the way it works (we get more bone-density improvement when used in a sequence including an anti-resorptive). Following this phase, patients are transitioned to an antiresorptive agent to help preserve the newly formed bone and maintain gains in bone strength.
Bone-building therapy represents a major evolution in the management of osteoporosis — shifting from merely preventing bone loss to reconstructing bone strength. For those most vulnerable to fractures, anabolic therapy offers not just protection, but the possibility of real recovery.
Who Should Consider Bone-Building Therapy?
Bone-building (anabolic) therapy is not a primary treatment for all osteoporosis patients, but for higher-risk individuals, it can be a critical intervention. It is most appropriate for those who face a significant risk of fracture, have already experienced multiple fragility fractures, or have a severely low bone mineral density.
In clinical practice, anabolic therapy is typically recommended for the following groups:
Patients with a history of osteoporotic fractures – individuals who have already sustained a low-trauma fracture, particularly at the hip, spine, or wrist, are at a significantly increased risk of subsequent fractures. Bone-building therapy can help restore skeletal integrity and reduce the likelihood of repeat injuries.
Individuals with very low bone mineral density (BMD) – a T-score of –3.0 or lower, especially when accompanied by other risk factors, may warrant anabolic treatment to rebuild bone quickly and prevent impending fracture.
Those who have failed or cannot tolerate antiresorptive therapy – some patients continue to lose bone density or suffer fractures despite being on bisphosphonates or other antiresorptive agents. Others may experience gastrointestinal side effects or skeletal complications like an atypical femoral fracture. For such individuals, anabolic therapy offers an alternative mechanism of action that actively promotes bone growth.
Postmenopausal women or older men at very high fracture risk – in this group, particularly those recently diagnosed after a fracture or showing rapid BMD loss, early initiation of anabolic therapy may offer better long-term protection than starting with anti-resorptives alone.
Patients with multiple clinical risk factors – tools like the FRAX (Fracture Risk Assessment Tool) help identify patients with a high 10-year probability of fracture. When combined with clinical judgement, these scores can guide decisions on initiating anabolic therapy.
It is also worth noting that bone-building therapy is most effective when used early in the treatment sequence for high-risk individuals. Starting with an anabolic agent followed by an antiresorptive medication has been shown to deliver better outcomes than the reverse sequence. A careful clinical assessment, including DEXA scan results, fracture history, and overall risk profile, is essential in determining eligibility.
What Are the Benefits of Bone-Building Therapy?
For individuals with severe osteoporosis or those at very high risk of fractures, bone-building (anabolic) therapy offers more than just disease control, it is the most potent therapy in restoring bone strength and reducing the risk of further injury. By actively stimulating new bone formation, this treatment addresses a core problem in osteoporosis. The following are the key benefits of anabolic therapy:
Active bone formation — anabolic therapy promotes the activity of osteoblasts, the cells responsible for building new bone, resulting in actual gains in bone mass.
Rapid improvement in bone density — patients typically experience faster and more significant increases in bone mineral density (BMD), particularly at the spine and hip—areas most vulnerable to osteoporotic fractures.
Fracture risk reduction — clinical studies have shown that bone-building therapy can reduce vertebral fracture risk by up to 86%, and non-vertebral fractures by approximately 30–40%, offering strong protection against future injuries with outcomes that are better than previously seen with anti-resorptive medications.
Improved bone quality — beyond increasing bone mass, anabolic agents help improve bone microarchitecture, enhancing both the strength and resilience of the skeleton.
Early intervention advantage — using anabolic therapy at the start of treatment, followed by antiresorptive medication, has been shown to be more effective in long-term fracture prevention than beginning with antiresorptives alone.
Improved mobility and independence — by preventing fractures, especially of the hip and spine, patients are more likely to maintain mobility, avoid hospital admissions, and continue living independently.
Bone-building therapy plays a crucial role in comprehensive osteoporosis management, particularly for patients with advanced disease. It represents a shift from merely slowing bone loss to actively rebuilding strength and structure — helping patients move forward with greater stability and confidence.
Are There Any Risks or Side Effects of Bone-Building Therapy?
While bone-building (anabolic) therapy offers significant benefits in reducing fracture risk and restoring bone mass, it is important to understand the potential side effects and safety considerations before starting treatment. These medications are generally well-tolerated, but as with any medical intervention, certain risks may apply depending on the individual’s health profile and the specific agent used.
Injection-site reactions — mild redness, swelling, or discomfort at the site of injection may occur, particularly with teriparatide, which is administered daily via subcutaneous injection. These reactions are usually temporary and resolve without intervention.
Transient increases in calcium levels — teriparatide can cause a slight elevation in blood calcium levels shortly after administration. While rarely problematic, patients with a history of hypercalcemia may require closer monitoring.
Cardiovascular considerations — romosozumab has been associated with a slightly increased risk of cardiovascular events such as heart attack or stroke in some clinical studies but this has not been consistent in studies and it’s true effect has not been confirmed. It is generally avoided in patients with a history of cardiovascular disease at least till further evidence is available.
Leg cramps, dizziness, or nausea — some individuals may experience mild systemic symptoms, including muscle cramps, light-headedness, or gastrointestinal discomfort. These are usually short-lived and manageable.
Osteosarcoma risk (theoretical) — in animal studies, prolonged use of teriparatide was linked to a small increased risk of osteosarcoma, a rare bone cancer. Although this risk has not been observed in humans at prescribed doses, therapy is limited to a maximum of 24 months over a patient’s lifetime as a precaution.
Not suitable for certain conditions — anabolic therapy may be contraindicated in individuals with metabolic bone diseases other than osteoporosis, unexplained elevations in alkaline phosphatase, or a history of skeletal malignancies or radiation therapy involving the skeleton.
Cost and accessibility — these therapies tend to be more expensive than antiresorptive agents and therefore are reserved for those at a higher risk of fracture.
Before initiating anabolic therapy, a thorough medical evaluation is essential to determine suitability with secondary causes of osteoporosis being ruled-out. Treatment is closely monitored through regular follow-ups and appropriate blood tests to ensure both safety and effectiveness throughout the course.
Supporting Bone Health Beyond Medication
While bone-building therapy can significantly improve bone density and reduce fracture risk, medication alone is not enough. For optimal outcomes, it must be part of a broader approach to bone health that includes lifestyle and dietary strategies. These complementary measures play a crucial role in preserving gains made during treatment and reducing the likelihood of falls and injuries.
Weight-bearing and resistance exercises — regular physical activity helps stimulate bone formation and maintain muscle strength. Weight-bearing activities like walking or stair climbing, combined with resistance training, are particularly effective in supporting bone density and improving balance. Dr. Dinesh mentions that resistance training helps fight age-related muscle loss too, an integral cause of frailty with ageing that predisposes to falls and fractures.
Balance and coordination training — exercises that enhance stability, such as tai chi, yoga, or physiotherapist-led balance work, can reduce the risk of falls, which are a major cause of fractures in individuals with osteoporosis.
Calcium and vitamin D intake — adequate dietary calcium supports bone mineralisation, while vitamin D enhances calcium absorption and contributes to muscle function. Patients are advised to meet recommended daily intake through a combination of diet/ sunlight and supplementation when necessary.
Smoking cessation and moderation of alcohol — smoking accelerates bone loss and impairs bone healing. Excessive alcohol consumption also weakens bone and increases fall risk. Addressing these habits is essential for long-term bone health.
Fall prevention strategies — making simple changes at home, such as improving lighting, removing tripping hazards, and using assistive devices when needed, can significantly lower the risk of injury. Regular vision checks and proper footwear also play a role in maintaining safety especially in patients with diabetes.
Together, these measures enhance the effectiveness of bone-building therapy and contribute to better outcomes over time. By combining medication with targeted lifestyle choices, patients can take proactive steps toward stronger bones, fewer fractures, and greater independence.
Final Thoughts — A Stronger Foundation Starts with the Right Treatment
Osteoporosis may be silent in its onset, but its consequences can be deeply disruptive — physically, emotionally, and socially. For individuals at high risk of fracture, especially those already living with the fear or experience of broken bones, bone-building therapy offers a vital opportunity to shift the course of the disease. IN patients with a high risk of fracture, anabolic therapy helps rebuild bone strength, restore structural integrity, and reduce the likelihood of future fractures better than other therapies.
But effective care goes beyond prescriptions. When bone-building therapy is combined with the right lifestyle measures — nutrition, exercise, and fall prevention — it becomes part of a long-term strategy to preserve mobility, independence, and quality of life.
If you or a loved one has been diagnosed with osteoporosis, or if you're concerned about your fracture risk, schedule a consultation with us. With a personalised assessment and the right treatment plan, you can regain your bone health and continue activities you enjoy, worry-free.
Anabolic therapy (like teriparatide and romosozumab) actively stimulates new bone formation by promoting osteoblast activity, unlike antiresorptives, which reduce bone loss.
Studies show vertebral fracture reduction of up to 86% and non-vertebral fracture reduction by 30–40%, with faster and more robust increases in bone density and strength than basic antiresorptives.
It is contraindicated in patients with metabolic bone diseases other than osteoporosis, unexplained high alkaline phosphatase, skeletal malignancies, recent radiation, or severe renal impairment.
Yes, anabolic treatments are effective in reversing bone loss in cases such as long-term steroid use, where bone breakdown is accelerated. Dr. Dinesh mentions that it must be started as early as possible as glucocorticoid-induced osteoporosis results in a rapid loss of bone in the first three months of therapy.
chat with us
Welcome to The Metabolic Clinic
Holistic Care for Hormones, Bones, and Metabolic Health
Dr Dinesh graduated with honours from Monash University, Melbourne in 2009, receiving the Prince Henry's Prize in Surgery. During his endocrinology training in Melbourne, he won the top registrar award at the Endocrine Society of Australia Clinical Weekend in 2016, followed by securing Australia's only Andrology fellowship in 2017. Upon returning to Singapore, he was the sub-speciality lead for adrenal, pituitary, and bone services at Khoo Teck Puat Hospital and established The Metabolic Bone Clinic.
A passionate educator, he served as Associate Programme Director for Endocrinology at NHG, training the next generation of endocrinologists, and received the NHG Teaching Award for Senior Doctors in 2023. An expert endocrinologist with proficiency in both general and sub-speciality endocrinology, he has an interest in longevity through improving cardiovascular risk, metabolism, bone health, and muscle loss prevention, with the ultimate aim of improving the number of healthy years in one's life.
10+ Years of Experience in Hormone & Metabolic Health
Founder of The Metabolic Bone Clinic in Khoo Teck Puat Hospital
Sub-specialist training with international experts in Melbourne, Australia
Clinical Interest in Longevity & Metabolic Health
START YOUR PERSONALISED HEALTH JOURNEY
If you’re not achieving your treatment targets, struggling with weight changes, fatigue, or unexplained symptoms—it’s time to take a deeper look.
Get clarity with a tailored plan built around you and improving your metabolic health.